Kudos to Dr. Stephanie Bamidele, who delivered our very first R3 Grand Rounds of the Academic year. Her topic? Calm in the Chaos: An Approach to Rapid Responses.
A recording of her excellent presentation is available HERE for your viewing.
And here are my notes:
Anyone who has worked in a hospital knows that rapid responses occur frequently in the hospital. But it hasn't always been that way! The concept of Rapid Response Teams emerged in the 1990s, modelled after Code Teams (which originated in the 1960s), as a standardized group of people expected to respond to a call for help before a patient requires a Code Team's assistance. The RRT goal is to intervene and respond to prevent major adverse events. And then make systems changes that allow for the next response to be even more effective.
Anyone can activate an RRT.
RRT may be activated for a number of reasons: vital sign abnormalities, nurse or family detection of clinical deterioration, a change in mental status, and more.
Specific clinical criteria may be used to designate a RR present minutes to hours before a serious adverse event:
- HR <40 or >130
- SBP <90
- Respiratory Rate <8 or >28
- Oxygen saturation <90%
- Change in level of consciousness
- Change in urine output (<100ml/4 hours)
Like a Code, any Rapid Response starts with the basics: A (airway), B (breathing), C (circulation) and goes from there. See these images for a very clear description of events that should occur in the first five minutes of a RR:
A | AIRWAY Assistance (call for help) Activate RRT Annunciate when providing key information Acquire Data Attend to patient until RRT arrives Access (IV) Assist as directed by team leader
|
B | |
As in all parts of life, communication is everything!
Dr. Bamidele reminded us that a standard way of communicating (in this case, following the hospital ISBAR model) is the best way to go. Doing so, ensures that all people present at a RR, have a clear understanding of what is happening and what is being recommended.
Okay, doctors, so, you are the leaders of the RRT, right? What do you actually do then to be an effective leader? Here are key steps, as outlined by Dr. Bamidele:
- Identify team members and roles: who is the leader? what are the roles? Does everyone need to be here. Start with a simple, "I am Dr. ____, and I am leading this RR"
- Crowd control: limit to 8-9 people max, including the leader (doctor), ICU charge RN, bedside/flor RN, respiratory therapist, and any necessary techs (lab, xray, etc). Send everyone else back to work.
- Set a calm and assertive and inclusive tone. Be respectful, willing to ask for help.
- Promote a flattened hierarchy: think aloud, step back, voice specific findings (e.g. glucose, x ray findings, response to narcan_, ask for suggestions and/or feedback
- Gather info via parallel processing (this is hard!): visual assessment, forming a plan, proposing an intervention
- Have situational awareness: don't miss the forest through the trees, integrate evolving information in real time, reinforce plan, gather suggestions
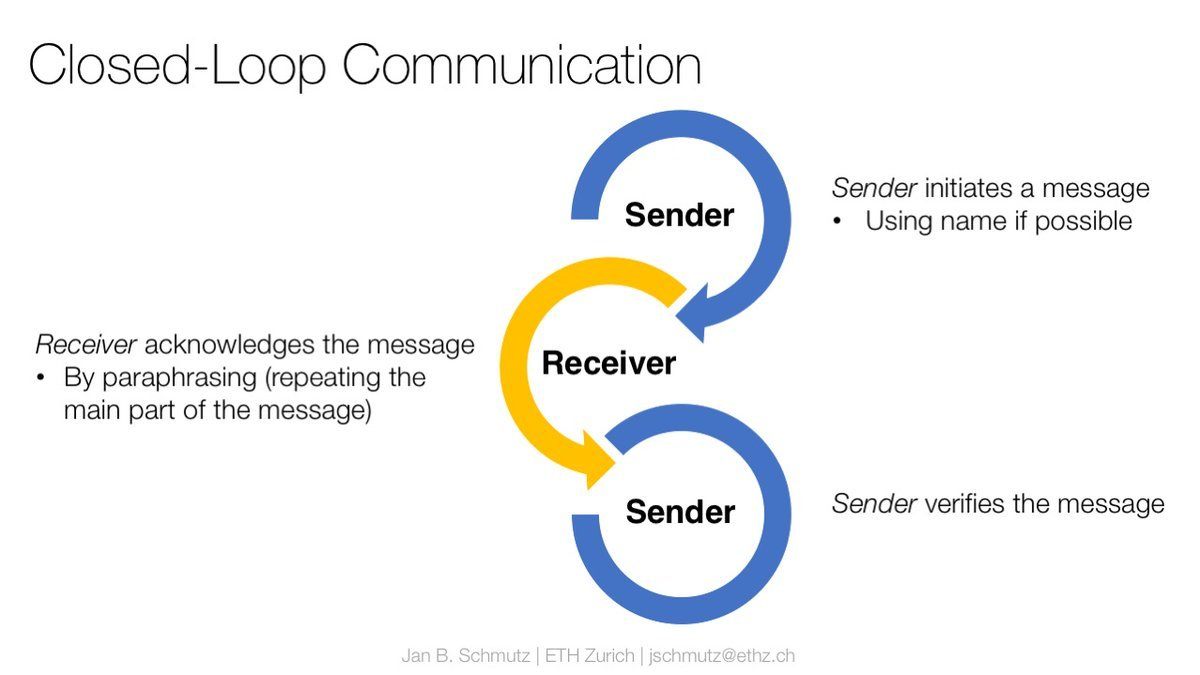
- Use closed loop communication: call out--> check back--> verification
Dr. Bamidele also gave us specific advice about the role of the Family Liaison during a rapid response or a Code event. There is mixed data on the harm/benefit of a family's presence at the bedside during these acute events, and so it is generally recommended that staff give the family the option of being present or leaving (without judgement). If the family is present, a designated staff person (RN, junior resident, etc) should be designated as the Family Liaison. That person should introduce themself, explain what is going on, stay by the family member's side (regardless of whether they stay or go), and provide that person an opportunity to ask questions.
The aftermath
Once the Rapid response is done, it is super important to debrief, says Dr. Bamidele-- for two main reasons: first, because a Rapid Response often occurs in intense situations that may have a lasting impact on the team and that may require emotional processing and reflection. Second, reflecting on the process will hopefully allow you to do a better job next time.
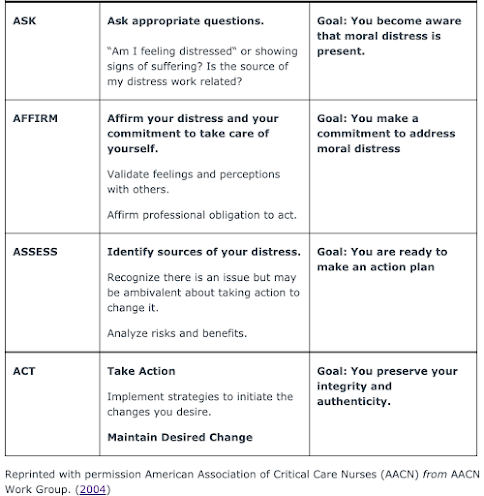
To address possible moral distress occurring in this context, consider the model of the 4As from the American Association of Critical Care Nurses (in graphic below)




No comments:
Post a Comment