A recording of the presentation can be viewed HERE.
There will be no Grand Rounds sessions on 12/28 and 1/4 due to the holidays.

A recording of the presentation can be viewed HERE.
There will be no Grand Rounds sessions on 12/28 and 1/4 due to the holidays.
A recording of the presentation can be viewed HERE.
A recording of the presentation can be viewed HERE.
A copy of Dr. Cooper's slides can be accessed with this link:
https://docs.google.com/presentation/d/1vsp0T3Qe4hllyvopmf694amcf5t8SJH2zVW0haJMMo0/edit?usp=sharing
A recording of the presentation can be viewed HERE.
A recording of the presentation can be viewed HERE.
A recording of the presentation can be viewed HERE.
A recording of the presentation can be viewed HERE.
A recording of the presentation can be viewed HERE.
Hello, Grand Rounds community of the Sutter Santa Rosa Family Medicine Residency Program. Often, within our systems of medical education, we unintentionally perpetuate frameworks of systemic racism and oppression if we do not actively seek to utilize a lens of Diversity, Equity, and Inclusion. Due to feedback received regarding bias and outdated racial inequity frameworks during the presentation “Evaluation of Suspected Cardiac Arrhythmias” by Dr. Moulton, our Didactics team and Residency leadership have decided to not share the link to the presentation. We have done outreach to Dr. Moulton regarding our concerns. We all continue to learn and grow as our understanding of racial equity and medical education expands. As a program, we are actively working to create a DEI Commitment for presenters with a DEI resources folder in order support our presenters in this important work. Once the resources are finalized, we will share the presenter folder here.
A recording of the presentation can be found HERE.
A recording of the presentation can be found HERE.
Many thanks for an excellent Grand Rounds year-- we covered a wide range of topics from Drowning Prevention to Moral Distress, from CKD to Gender Expansive Care, from Racism in Medicine to Bias in Documentation, from Breast Cancer Reconstruction to Alcohol Withdrawal. And more!
Also thanks to our last Grand Rounds speaker of the year, Dr. Vanessa Pinto, who gave an excellent talk on Marijuana (MJ) in pregnancy and postpartum.
A recording of her presentation is available HERE.
My notes:
Many thanks to Dr. Alec Ludwig for an excellent presentation about liver and biliary abnormalities in pregnancy. It was jam-packed with good information.
A recording of his presentation is available HERE.
My notes:
Remember that what we typically call "liver function tests" is actually a misnomer. In fact, there is no test that reliably demonstrates the liver's function. Elevation of AST and ALT -- the liver enzymes-- indicates liver injury, not liver dysfunction. Albumin and prothrombin time are factors that are produced by the liver and may be better markers of function.
In normal pregnancy, you can see elevated alkaline phosphatase (up to 3x normal), as well as elevated cholesterol, triglycerides, and fasting gallbladder volume. Note that many measures we use to evaluate the liver (AST/ALT, T Bili, PTT, liver size, bile acids) don't change in pregnancy.
Hepatocellular injury as measured by elevation in AST/ALT:
Gallstone disease in pregnancy
Gallstone disease is much more prevalent in pregnancy for several reasons. 1) Increased estrogen levels increase cholesterol, thereby supersaturating bile with cholesterol. 2) Progesterone slows contraction of gallbladder, disrupting the excretion of bile acids. AND 3) Increased fasting gallbladder volume.
Generally treat GB disease in pregnancy with IV antibiotics, surgery if indicated. Laparoscopic cholecystectomy is safe in pregnancy, safest in the second trimester. Should occur within 24-48 hours conservative management. ERCP is also safe in pregnancy; minimize radiation by shielding, fetal monitoring.
Viral Hepatitis (A-E)
Many thanks to our SoCo Public Health Officer, Dr. Sundari Mase and our SoCo Vaccine Chief, Dr. Urmila Shende for an excellent Grand Rounds this week on Pandemic Pearls and Pivots: A Public Health Perspective.
A recording of their presentation is available HERE.
As we all know, COVID-19 has taken a great toll on our world, our nation, and our county. As of this week, there have been 6.28 million deaths worldwide (probably an underestimate), >1 million US deaths (more have died from COVID-19 than HIV/AIDS, the 1918 influenza pandemic), 90,000 deaths in California, and 491 deaths in Sonoma County. This has led to the largest drop in life expectancy since WWII. And we know that there have been disproportionate numbers of cases, hospitalizations, and death among people of color.
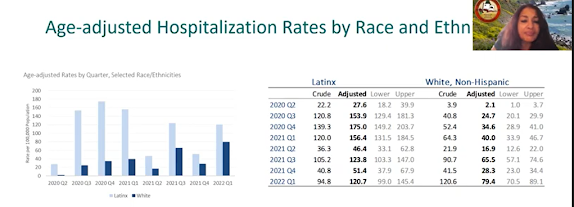
 Vaccines work! The reduce infection, hospitalization, and deaths.
Vaccines work! The reduce infection, hospitalization, and deaths. |
| from https://socoemergency.org/ |

If you are interested in this week's Grand Presentations Be Curious: Cultivating Curiosity in Learners, Teachers, and Practitioners of Family Medicine, a recording is available HERE.
I will be brief with my notes:
I presented Dr. Todd Kashdan's model for the 5 Dimensions of Curiosity:
“Curiosity is fundamental to our physicianship, and serves both the art and the science of medicine. (How do you do? What’s your name? Where do you come from? How do you feel? Tell me more about this pain you’re having…). Curiosity is how we explore the world, this primal “wonderment” that stimulates exploration, engages both the human imagination and human intelligence. Both are integral to the humanities and science, as well as the synthesis of the two, which is clinical medicine.”https://www.bumc.bu.edu/facdev-medicine/files/2010/09/Fitzgerald_AnnInternMed_1999_130_70_Curiosity.pdf
I also shared with you a model created by an Israeli hematologist, Dr. Shattner, in his essay from 2015 on Curiosity in medicine. His model (which I don't love aesthetically but adore in its core tenets) espouses that curiosity is good cognitively and emotionally, and it's good for patients and physicians.
You can see his model below and an updated rendition below (by yours truly)
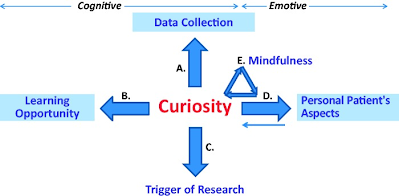 |
Shattner, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4484215/ |

Thanks to our speaker this week, cardiologist Dr. Joanne Tsai, for an excellent review of cardiology topics for outpatient care of cardiology patients, particularly regarding Atrial Fibrillation and Atrial Flutter.
A recording of her presentation is available HERE.
My notes:
 |
| pseudo atrial flutter |

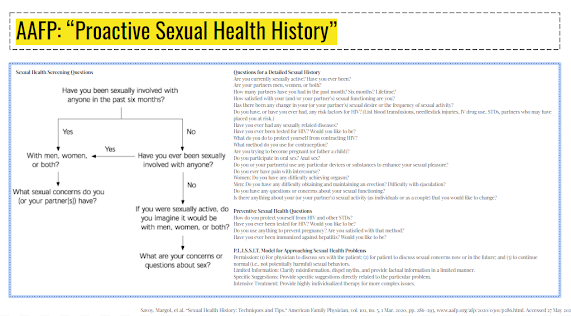
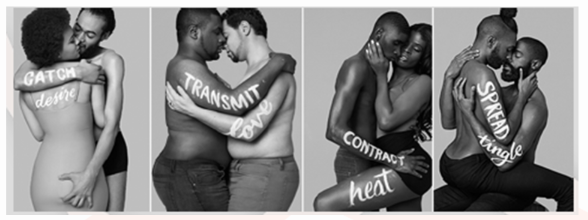
Big thanks to Dr. Sophie MacArthur for her excellent presentation on a topic that we could ALL use a little education on-- Sex. And specifically how we talk about it with patients.
The recorded presentation is available HERE.
Link to her slides is HERE.
My notes:

STIs: Not just condoms - frequent testing, PrEP or PEP, etc.
Contraceptives: RHAP Birth Control Options Fact Sheet; bedsider.org
Consent: Yes, No, Maybe Inventories
Painful sex: Mayo Clinic resources
BDSM/Kink safety: San Francisco Aids Foundation S&M and Kinky Sex Resources; NCSF Kink Aware Professionals Directory
Legal: National Coalition for Sexual Freedom Incident Report; safewordtax.com
I am personally feeling very grateful to Dr. Onna Lo for a really lovely presentation this week on Gratitude, Happiness and Resilience. I have already integrated some of her techniques. . .priming my day and granting myself a "celebration" list (what I have accomplished in the last 24 hours) rather than a "todo list" (all the things I feel bad about not accomplishing).
If you are interested in watching her presentation-- and you should be -- it is available HERE .
Here are my notes. sorry they are brief:
Dr. Lo encouraged us to start every day and every encounter with the ABCs:
A: Awareness (ground yourself)
B: Body/breath (be in your body, find your breath)
C: Connection (with your surroundings, yourself, your patients)
People are struggling
Something to strive for -- Dr. Lo recommends in our own lives and for patients. To be: Empowered, Engaged, Excited, and Embodied
Some definitions:
Lesson #1: A positive mindset sets you up for better learning
A positive mindset leads to better learning, improved performance, better problem solving
In The Happiness Advantage, author and researcher Shawn Achor, proposes that personal happiness leads to professional success (not vice versa). Happiness is a choice. Happiness spreads. Happiness is an advantage. Read more about his work here.
The happier you are, the more successful you will be (Horn & Arbuckle).
Gratitude predicts hope and happiness more than forgiveness and patience.
How can YOU build happiness? 21 days in a row x 2 minutes >> 3 gratitudes, positive journaling
Lesson #2: Our brains tend to get stuck in negativity
Half glass full or half empty?
Dr. Lo showed us a series of sociological experiment in which people consistently chose the negative response consistently after being primed with a negative response, even when the outcome was quite positive. If primed with the positive response, people were more likely to choose positive.
We can unstick ourselves by "priming"-- that is, retraining the mind first thing in the morning with gratitude. That is, starting the day positive allows for the day to be more positive.
Exercise: Draw a triangle, write down 3 gratitudes (these must be heartfelt!)

2) what I am grateful for in others
3) what I am grateful for in my current situation
Exercise: Draw a triangle, write down 3 wonderful things that you accomplished in the last 24 hours (this is your celebration list)
Exercise: Draw a triangle: write down 3 things that will make today great

Lesson #3: There is science supporting positivity and gratitude
Coherence=optimal coordination between the heart and the mind ==> heartrate variability is a really beautiful sinus curve in someone who is completely in a coherent state. Being in this mindset is better for your whole body.

Much more information about coherence and Heart Math at the Heart Math Institute Website found here.
Exercise:
1) Heart focused breathing: 5 breaths in/5 breaths out (requires nothing more than the breath)
2) Inner coherence: use positive emotions or feelings of gratitude to establish a coherent beat (using heart math monitor)
And finally, keep a gratitude journal. Even in these hard times, there are big and small things to be grateful for.
Many many thanks to Dr. Ritch Addison for his wonderful Grand Rounds this morning (and his 40+ years of teaching and mentorship at Santa Rosa Family Medicine Residency. It felt like a warm cup of perfectly brewed tea to sit and listen to Ritch share his observations from the professional socialization of family physicians.
For those of you who missed it, the recorded presentation is available HERE and is definitely worth watching!
I have jotted down just a few notes. The talk is definitely best absorbed by listening/watching.
To start, Ritch asked us to consider what resonates with you?
A long time ago (40+ years) in a galaxy (not so) far far away, Dr. Ritch Addison followed nine family medicine interns around for three years-- "I wanted to see what they did." His notebook always in hand, Ritch took call with them, observed them delivering babies, suturing folks in the ER, race to clinic, etc. For three years, he watched them live and process their entire residency training experience.
Today's talk was a summary of observations and models derived from that research. Ritch highlighted a number of important themes:
Surviving residency involves a TON of immediate issues that new R1s are confronted with
Working relationships are a complex piece of residency identify formation. Relationships with:
Spheres of existence evolve over time
work education life outside
initial purpose/weight take care of patient learn family medicine maintain some QOL
evolves into GET done do procedures whatever is left
There is an inherent conflict and contradiction between a resident's ideals/goals/visions (expectations) and the everyday practices of being a resident.
Ritch finished off with his assessment of the "modes of surviving"
Over-reflecting: too much self reflection (favorite patient dies, yelled at by attending, make a mistake)
Covering over: using little self-reflection, so focused on what you are doing you cannot see what is happening to you
Moving between these two takes wide movements and is extremely jarring. How do residents learn to move between these modes? Ritch said clearly that it's really NOT about finding the sweet spot of reflection, but rather being able to smooth out the space and integrate these two forms of being.
Finally, Ritch introduced the birth of the Personal and Professional Development groups (P&PD) that really were birthed from the desire of residents to facilitate the movement between these two spaces-- to smooth it out. After all, everybody feels the same way. What happens when we talk about our experiences? We start to resolve the two modes. . .
Ritch ended with an excerpt from The Heroes Walk, by Anita Rau Badami on the physician-patient relationship. Listen to him read it at the end of the recording. That is what family medicine is all about, right? The most meaningful way we can bring health to people.
Many thanks to Dr. Navid Pourtaheri, new-to-our-community plastic surgeon, on Skin Cancer and Skin Cancer Reconstruction. This is a great summary of skin cancer findings and some specific indications and recommendations of when to involve plastic surgery.
A recording is available HERE
Skin cancer types: basal cell (BCC) squamous cell (SCC) keratoacanthoma, melanoma
Basal cell cancer (~4 million cases/year in US)



Many thanks to Dr. Julissa Lopez for her important Grand Rounds presentation on LGBQT+ Fertility and Preconception Counseling. Key take home message up front: primary care physicians SHOULD be helping LGBQT+ patients pursue the families they desire. It's definitely within our scope.
If you would like to watch, the presentation is available HERE.
Dr. Lopez started with a reminder of the wide range of gender and gender identities that we may encounter. Refer to the Flying Gender Unicorn graphic below as often as you need to to remind you of the range of gender identity, gender expression, gender expression at birth, sexual identity, etc (and to help your patients and you better understand themselves).

 |
| https://www.lgbtmap.org/equality-maps/foster_and_adoption_laws |
 |
| https://www.obgynofatlanta.com/iui |
Thanks to Dr. Robledo for an excellent review of AUD and AWS at Grand Rounds this week. A link to a recording of the presentation is HERE.
Note: in place of male/female to discuss gender differences, Doctor Robledo used "assigned female at birth" (AFAB) and "assigned male at birth" (AMAB). These abbreviations are included in this summary.
Alcohol use

Risky alcohol use is drinking that can lead to health consequences and may develop into alcohol use disorder.
Alcohol use disorder is a pattern of drinking that significantly impairs health and functioning.
Binge drinking: drinking in a way that increases blood alcohol level >0.08 in 2 hours, generally >4 drinks at once for AFAB, >5 drinks at once for AMAB
 |
| https://creativecommons.org/licenses/by/4.0/ |
 |
| https://www.aafp.org/afp/2013/1101/p596.html |
 |
| https://www.aafp.org/afp/2002/0201/p441.html |
 |
| https://www.clinicaladvisor.com/home/topics/psychiatry-information-center/alcohol-withdrawal-individualized-care-and-pharmacologic-treatment/ |
 |
| PAWSS, Maldonado 2015 |
 |
| SAWS: https://www.aafp.org/afp/2013/1101/p589.html |
 |
| https://www.aafp.org/afp/2016/0315/p457.html |
A recording of this presentation is available HERE . *** Thanks so much to Dr. Kendal Hamann, SMGR Endocrinologist, for an outstanding Gra...