***
Many thanks to local psychiatrist, Dr. Alex Threlfall for an excellent Grand Rounds presentation this week: Addressing Benzodiazepines in Primary Care. As we all know, benzodiazepines (heretofore BZD) play a major role in the national opioid epidemic, and despite lack of organized attention to the issue, addressing concomitant BZD use and misuse is an important public health and safety issue for all our patients.
My summary:
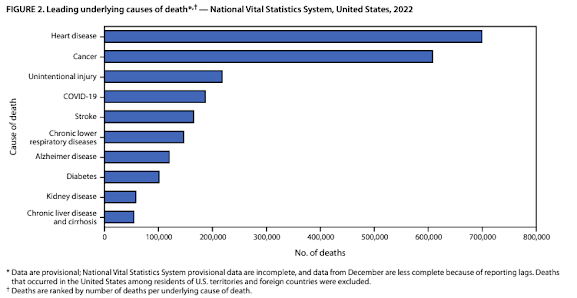
BZD were historically the number one prescribed medication in the world (in 1960s and 1970s). They are frequently involved in opiate overdose deaths. The combination is very dangerous. After opioids, BZD are the most commonly caused agent involved in intentional and unintentional overdoses.

History of:
- Mental health conditions associated with trauma
- Substance use disorder (SUD)
- Elderly (>65)
- Chronic pulmonary disease (e.g. COPD)
- Women of child-bearing age
- Chronic pain (with or without opiate use)
Trauma
Trauma is rampant in our patient population, upwards of 20-50% of the general US population report a history of childhood physical or sexual abuse. It's even higher -- 70%-- in populations with depression/anxiety, SUD, chronic pain and functional pain disorders like IBS. Sexual abuse directly influences development of SUD.
**THERE IS NO EVIDENCE SUPPORTING THE USE OF BZD in TRAUMA or PTSD (either acute trauma or long term treatment). In fact, there are studies that suggest that adding benzos at the time of a traumatic event can increase PTSD, can lead to addiction, and that benzos can even reduce the efficacy of psychotherapy by blunting therapeutic effect.

Benzodiazepines are highly addictive.
VA data from 2016 shows that 58-100% of patients prescribed BZD will become physically dependent, 50% of patients with a pre-existing SUD will develop a BZD use disorder, and 5-10% of patients newly on BZD will develop SUD.
Benzodiazepines are particularly risky for older adults.
We have not paid attention to our patients as they have aged. People prescribed a BZD were often not offered a safer alternative. In a study of geriatric patients on BZD, <1% had been referred for psychotherapy, 10% were co-prescribed an opioid. The most common indication for BZD in these patients were insomnia and anxiety. Despite this evidence of harm, population studies show increasing rates of BZD rx in elderly patients and failure to discontinue, particularly in people >80 years old and Trend women>> men.
 |
| All adults on new or continuous BZD rx |
The older you are, the more likely you are to be on a BZD. This is a problem. White people have "better access" to BZD than their non-white cohorts and higher rates of BZD misuse.
Risks of BZD are real.
Falls, hip fractures, sedation, cognitive impairment, motor vehicle accidents. While an observational study from ~10 years ago found that being on BZD, people were more likely to develop dementia. It is not true that BZD causes dementia, but it does cause cognitive impairment. All BZD are on the Beer's list of medications not safe for elderly patients. Number needed to harm is 2: for every person you successfully treat with BZD, you will harm two.
As in everything, prevention in the best strategy. In other words, avoid new starts of BZD.
Okay, so when are BZD actually indicated as first-line therapy?
- Acute crisis setting (e.g. patient floridly manic, psychotic, agitated patient => 2mg lorazepam)
- Bipolar mania
- Severe panic
- Alcohol withdrawal (though we are moving away from BZD use)
- Seizure disorders
- Procedures & planned events (e.g. for patients with intellectual disability who need sedation)
- Phobias (e.g. flying, but beware)
If prescribing BZD for these conditions, you should use the lowest effective dose, avoid alprazolam (aka xanax) whenever possible (super short, very fast acting, too much reinforcement) and restrict prescription for 2 weeks or less.
Of note, BZD are THIRD line treatment for anxiety
First line is pharmacotherapy -- SSRI, SNRI-- and/or evidence based psychotherapy (CBT, mindfulness).
- SSRIs/SNRIs are all effective for anxiety disorders. Dr. Threlfall's favorites are escitalopram and sertraline. Start super low (2.5 or 5mg escitalopram=> target 5-20mg 25 mg sertraline, target 100-200mg). People with anxiety will often respond sooner than with depression. If they tolerate, will respond within 1-2 weeks.
- Part of efficacy is you! You need to reassure patients, check in (1 week to be sure started/tolerating), then see again in 2-4 weeks. You hold them psychically through the process
- Buspirone can be effective either standing or PRN. Literature doesn't do it justice. Titrate 10-30mg TID. Watch for serotonin syndrome.
- uses for Vets for prn to cross the GG bridge, take prn
- It's not sedating, but still helps with anxiety.
Second line: gabapentin>>pregabalin>>propranolol>>clonidine
amitriptyline*>>nortriptyline
hydroxyzine*>> diphenhydramine
- clonidine for pts with extreme anxiety 0.1mg TID can be pretty effective (BP and adherence and rebound BP issues). Can use 0.1mg patch, can co-treat hypertension
- *DON'T use amitriptyline in EVER elderly b/c of anti-cholinergic effects
- *DON'T use hydroxyzine and diphenhydramine in older adults >65 (people with cognitive impairment). Effects wear off pretty quickly, get tolerant quickly
Another note, BZD is NOT FIRST LINE TX for INSOMNIA (per all professional societies)
First line
All recommend CBTi as first-line treatment for insomnia
VA has a free app, free to download, easy to use, is effective: "CBTi coach"
 |
| Free app from the VA |
- Melatonin: 1-2mg max (long acting)
- Prazosin (if nightmares/trauma or waking startled): 1mg to start, up by 1mg every 4 days, as much as tolerated, stop at 3mg to see again. VA says 12-18 is safe dose (Threlfall maxes out at 8mg). Side effects: orthostasis, sedation, congestion
- Trazodone, low dose, start at 25mg, rarely go about 150mg. Above 200mg getting into anti-depressant range. Can get serotonin syndrome if on SSRI. People don't like hangover effect
- Mirtazapine: more sedating at lower dose 7.5-15mg, above that lose the sedation effect (but keep increased appetite). People when starting mirtazapine can experience heavy sedation during the day for 3-5 days. Try it when that sedation is not going to be too bothersome. Restless legs
- Doxepin: recent study 3-6mg safe and effective in older adults. On Beer's list, anti-cholintergic but at low dose, better safety profile
- Amitriptyline/nortriptyline
Third line
- Hydroxyzine, diphenhydramine
- Ambien (Zolpidem) or Temazepam if you really need to, particularly if concomitant bipolar disorder
How to initiate BZD:
1. Rare if you ever do
2. Short symptomatic relief 1-2 weeks
3. Get psychiatry consult
4. Make sure you have the conversation with the patient, "This is going to be short term"
5. Be very clear about the risks
6. Discuss exit strategies (taper, switch)
7. Be the only prescriber
8. Document failure of other trials of meds
9. CURES, urine drug screen
10. BZD treatment agreement if going more than 2 weeks
Use these only Total Daily Dose (TDD): Lorazepam 2mg TDD, Clonazepam 1.5 TDD, Diazepam (he doesn't like, people seek out the effect, 15mg TDD), Temazpeam 30mg TDD
There is evidence that if patients are informed of the risks of BZD, they want off them. In one study in which pharmacy sent patients taking BZD information on the risks of BZD: 62% self-started BZD taper, 21% were completely off at 6 month follow-up. Give people the opportunity to get off with education, encouragement and support.
One final note, getting people off BZD is not not without risk. In fact, there is new evidence that there is real risk in discontinuing BZD. When people are taken off BZD, they die more, fall more, go to the hospital more, have more suicide attempts and non-fatal overdoses. We have to pay attention to the effects of long-term BZD on their neurophysiology. When people are really attached, get them on the lowest dose possible. And don't use them every day -- intermittent use is MUCH safer than chronic use.

Tapering is a team-based approach. Use your nurse, your MA, a colleague, behavioral health. Don't start right away. Establish relationship. You ARE the medicine in the room. Establish that before making any changes. It goes a long way.