
A recording of this presentation can be found HERE.
***
Many thanks to Dr. Grimley, who gave their senior Grand Rounds presentation on a topic that most of us would be nervous to touch with a ten-foot pole -- alternative sexual lifestyles -- also known as "kink" and "BDSM." Dr. Grimley shared the prevalence and range of alternative sexual practices in our country and showed data about how people's sexual behavior influence health, illness, and experiences of the healthcare system (no surprise). Many healthcare providers don't know enough about alternative sexual practices to even begin a conversation, much less to be able to provide comprehensive care. Ultimately, they encouraged us to not shy away from learning about all the kinds of sex our patients are having so that we can better serve them.
First, let's define "kink" --the practice of unconventional or unusual sexual preferences or behaviors, fantasy or desires. These are behaviors that are influenced by political leanings, cultural upbringings, and religious beliefs and vary widely among individuals. What about "BDSM"? The BDSM Triskelion, created in the 1990s defines the three pillars of BDSM: Bondage and Discipline, Domination and Submission, Sadism and Masochism. But there are many other "kinks" outside these tenets. And not all of them are sex-related
Dr. Grimley started by laying out the dominant "sex hierarchy" -- reading a passage from a 1984 piece by Gayle Rubin's "Thinking Sex: Notes for Radical Theory of the Politics of Sexuality.
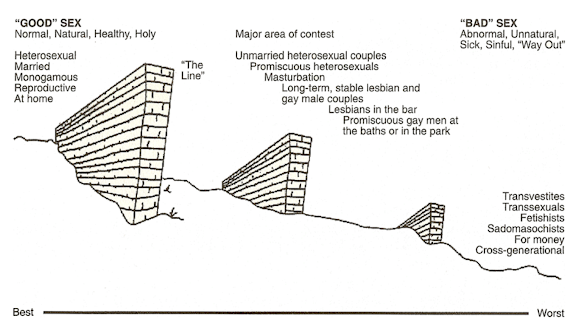
"Good" sex according to this hierarchy is heteronormative, monogamous, home-based sex. "Bad" sex is trans-sex, fetish-sex, public sex. If we, as healthcare providers, are acculturated to accept these norms, then we tend to disregard a decent subset of the population that engages in alternative behaviors, and in so doing, miss opportunity to improve people's health. From this perspective, there may be an uninformed assumption that kink is happening without consent and is potentially harmful to participants. These are biases we carry.
In fact, Dr. Grimley said, every interaction in the kink community must be grounded affirmative consent (i.e. "opt in"-- we talked about what was going to happen before it happened and I agreed that I want to participate), rather than the more traditional, heteronormative "opt out" (i.e. person pushes forward with sexual advances without aforementioned conversation, participant is supposed to say "no" if they don't want to mid-act).
Core principles of kink:
- Consent: mutual, iterative, can be revoked at any time, enthusiastic yes!
- Pre-negotiation: talk about everything
- Community: strong cultural values (see above), historic roots, and social networks that guard against violence/abuse
- Knowledge
- Producing good experiences
Here are some important terms to learn in the kink community:
- safe word: a word agreed on before the sexual act beings that, when spoken, stops any sexual act/scene immediately
- scene: a kinky encounter or experience, often planned in advance, that can last for minutes, hours or days
- aftercare: time and attention given to partners after a scene is complete
- drop: a feeling of mental or physical exhaustion after a scene
- hard limits: what someone will absolutely not do, does not want to do
- soft limits: a behavior or action someone is hesitant to do but may try
- munch: a public meet up of people in the kink community
- roles: top/dominant/dom/domme/sadist + bottom/submissive/sub/masochist
- dungeon: a room or venue specifically for BDSM activities
- play: kinky activities or interactions
- toys: implements or tools
- edge play: greater risk, higher intensity, or considered more transgressive than common play

After giving us a education on the vocabulary and core principles of kink, Dr. Grimely went on to share with us some of the statistics showing kinksters as an unrecognized sexual minority. But activities associated with kinking are perhaps less rare than you might suppose: 21% of participants in the 2015 Sexual Exploration in America Study had been "tied up", 15% had participated in "playful whipping", 31.9% reported "spanking" during sex, and 3.4% reported having gone to a BDSM party or dungeon. In another study, sponsored by Durex condoms, 10% of participants reported SM and 36% bondage in their sexual acts.


- Risks in bondage: rope constriction, strangulation and circulatory issues. Risk mitigation includes bondage release methods, soft rope, breaks to allow for circulation (after 20-30 minutes), never leaving someone unattended when bound, stopping immediately in the case of loss of sensation, and even using a squeaky toy to stop/drop as a non-verbal communication
- Risks in impact play of unintentional injuries. Risk mitigation includes hitting fleshy and fatty areas (buttocks, thighs, calves); avoiding and watching out for "wrapping", and cleaning and dressing any broken skin
- Risks of wax play: skin issues, burns, and unintentional fire. Risk mitigation includes moisturizing skin and/or shaving hair prior to wax play; not wearing flammable perfumes or colognes, avoiding skin that is already problematic (eczema, psoriasis), choosing the correct materials (bees wax burns the skin, shea butter or soy is safer and lower heat)
- Risks of electricity play: not suitable for those with heart disease or electronic device or implant, not suitable with water/fluids, avoid mucous membranes, care with metal piercings
- Risks of breath play: very high risk and potentially deadly. Risk mitigation: avoid using anything other than a hand, never put pressure on the windpipe, never do breath play alone.
Fetlife: https://fetlife.com/
National Coalition for Sexual Freedom’s “Kink and Polyamory Aware Professionals (KAP) Directory” http://www.ncsfreedom.org/key-programs/kink-aware-professionals-59776
The Network / La Red - http://tnlr.org/en/
National Coalition for Sexual Freedom (NCSF) http://www.ncsfreedom.org
The Alternative Sexualities Health Research Alliance (TASHRA) https://www.tashra.org
Community-Academic Consortium for Research on Alternative Sexualities (CARAS) https://www.carasresearch.org
Kink Knowledgeable http://training.kinkknowledgeable.com
Diverse Sexualities Research and Education Institute https://dsrei.org
Multiplicity of the Erotic Conference (MOTE) https://www.mote-con.org



No comments:
Post a Comment