
A recording of this presentation is available HERE
***
Many thanks to Dr. Danny Toub, who gave an excellent Grand Rounds presentation this week titled Colorectal Cancer Screening: What PCPs need to Know. A recording of the presentation is available above.
My notes:
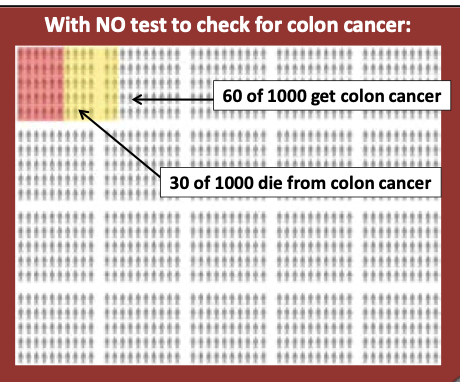
Colorectal cancer (CRC) is the #2 cause of US cancer deaths overall in men and women, the #1 cause of cancer death in men under 50. In 2024, we are predicted to have more CRC deaths than COVID deaths. In theory, CRC is an ideal disease to screen for because the slow development from polyp to cancer -- on average, 10 years -- means that early detection can actually lead to lives saved; if caught early, death can be prevented.

Through many efforts, we have increased our CRC screening over the last two decades, and in doing so, we have decreased CRC mortality. Unfortunately, it's not by a lot: a 2023 study published in JAMA, found that CRC screening only extends a person's life by an average of 110 days (see forest plot below).

It is important to note, however, that current quality measures do incentivize us to screen for CRC-- there are payments attached to our doing so, through both state and federal programs. So, to be clear, we screen to 1) decrease CRC mortality and 2) because our systems are set up to do so.
How do we screen?
Many of us are well aware that there are several CRC screening modalities, which are essentially considered equivalent in terms of CRC detection rates:
- q10 year colonoscopy (most invasive, most cumbersome, but benefit of being able to remove polyps during the procedure)
- Annual FIT test (has replaced the older FOBT test)
- stool DNA tests (frequency variable)
- q5 year flexible sigmoidoscopy (screens less of the colon but does not require anesthesia and can be done by primary care clinicians, if trained)
- Emerging serum tests (not yet FDA approved)

Current USPSTF Guidelines (2021) recommend shared decision-making to decide which modality to use; there are a number of studies showing many different screening tools decrease CRC mortality (with colonoscopy slightly better than the other modalities in detecting cases and averting death). More invasive screening tools have more serious potential harms, but all positive screening tests lead to colonoscopy, as the gold standard for diagnosis of CRC. Of note, there is a lack of screening colonoscopy access in our county, and most of the community health centers (and even Kaiser) default to non-invasive screening via FIT testing. As an aside, SRCH is moving to a pilot program screening with a more expensive DNA FIT testing q3 year (rather than q year) starting next month.
Who to screen?
Current USPSTF Guidelines (2021) make a Grade A recommendation for all adults 50-75, with a Grade B recommendation for adults 45-49. They make a Grade C recommendation for people 76-85 with shared decision-making based on 10 year life expectancy (i.e. healthy 76+ year adults should be selectively screened).
Whereas there is a statistical benefit to screening people 45-49, the AAFP actually disagrees with the USPSTF and recommends screening starting age 50 with "insufficient evidence (I)" to recommend screening before then. The 2023 ACP guidelines are slightly less in terms of screening frequency, recommending a q2 year FIT test (vs 1 year per USPSTF).
What works?
Dr. Toub spent some time talking about how we get patients to get screened -- possible interventions include one on one conversations, client reminders, group education, provider prompts, navigation, EHR enhancements, but in the end, Dr. Toub advocates for all kinds of ways:
- give nudges
- use decision aids
- give options (not too many)
- tell stories
- make personal recommendations
- send serial text messages
For more ideas, see some of the images below. Also note that The Community Guide , supported by the same folks who sit on the USPSTF and gives evidence-based recommendations for what works to improve population health, recommends making sure that materials in given in the correct language, that transportation assistance be made available, and that dedicated patient navigation helps in low-resourced settings-- increaseing rates of colonoscopy and FIT by 13 and 12 percentage points respectively.



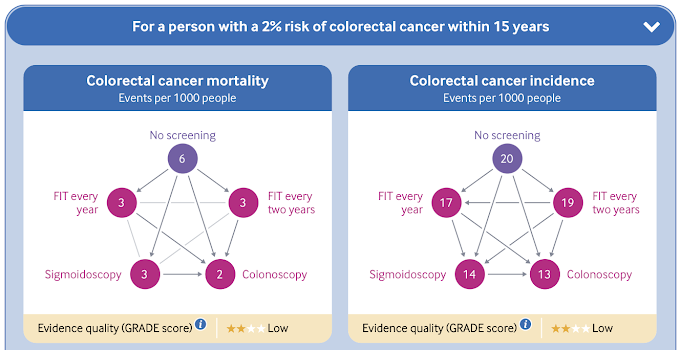
Dr. Toub ended his information-packed presentation with the suggestion that maybe we are thinking about CRC screening all wrong. In some well-resourced countries with national health plans, CRC screening is approached differently: rather than screening EVERYONE over a certain age, this BMJ guideline, published in 2019, suggests using a risk-based calculator to determine who should be screened. This suggests NOT screening anyone with <3% 15-year risk (based on this RISK CALCULATOR), which takes into account age, smoking and alcohol use, BMI, cancer hx among other things) to calculate that risk. IT also uses decision aids to help in determining screening decisons (see below):
It's AI, of course! Watch the last few minutes of Dr. Toub's talk for breaking news on AI in CRC screening. I think I'll leave it out of my summary today, as it is all still just starting and not really moved into standard practice.
For now, remember these take home points: 1) CRC screening decreases deaths from CRC but does NOT improve all-cause mortality, 2) multiple screening modalities at multiple different intervals are considered equivalent, so use shared decision-making with your patients to meet their needs, and 3) use lots of different nudges to get your patients to follow-up with screening, but don't forget to mention the importance of CRC screening yourself!
Until next week. . .


No comments:
Post a Comment