
Many thanks to Dr. Desiree Carmen for an evocative Grand Rounds presentation this week entitled Dismantling the Healthcare Hero. A recording of her presentation-- definitely worth your time and attention-- is available HERE.
Dr. Carmen took the hour to explore the notion of heroism as it applies to medicine. She asked us to question why we liked being called heroes at the start of the pandemic and why that may not feel so good right now-- a year and a half later. And she challenged us to propose alternative narratives to support the systemic change that so many of us wish to see.


Dr. Carmen showed us now-familiar images of healthcare workers as masked altruistic protagonists. As the world shut down in March 2020, she began, we felt the love from companies-- free vacations, discounted goods. . . stories of NYC meeting at 7am to clap for healthcare workers. It felt pretty good to be healthcare hero.
Our egos, after all, were not averse to the notion that we could be heroes. We signed up for this! For physicians, we took the Hippocratic oath; for nurses, the Nightingale pledge. We adhere solidly to notions of altruism, beneficence, justice, non-abandonment and solidarity. And we want to serve.
But, she explained, I wanted to know why society wanted us to be heroes.
Dr. Carmen showed us 3 hero archetypes that Americans particularly admire:
- The Everyman Hero: this is the person with no special skills, one for whom life has thrown an adventure at them, asked to do heroic deeds
- The Classical Hero: someone with special abilities and/or skills that puts them above others in the society and grants them their positionality as hero due to those skills
- The Epic Hero: the person with a noble birth story, larger than life



Dr. Carmen segued from these hero archetypes into the work of James Opie Ursom, a mid-century philosopher who wrote about the supererogatory: that is, morally excellent actions that go beyond the duty of the agent-- more than is asked for. All heroic actions are supererogatory, but not all supererogatory actions are heroic. Heroism involves known involvement with risk. i.e. we must CHOOSE the risk. Well, did we?
Risk has not been in short supply during this pandemic.
But PPE has.
PPE Shortages: We all are well aware of the experience of working without a feeling that we had adequate PPE (e.g. reusing N95s, gowns, etc). This is not unique to this pandemic; it has, unsurprisingly, been experienced in epidemics prior to this (including ebola, SARS, H1N1)
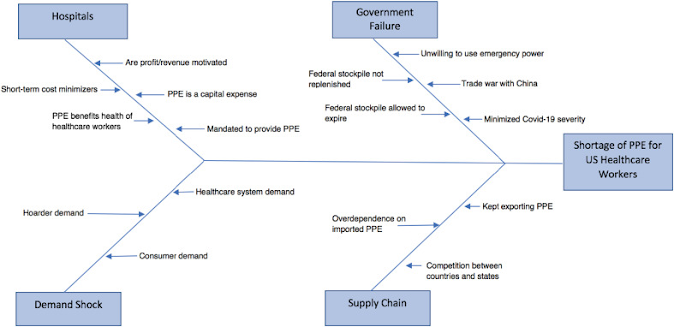 |
Recreated Figure 1 from Cohen J, Rodgers YVM. Contributing factors to personal protective equipment shortages during the COVID-19 pandemic. Prev Med. 2020;141:106263. doi:10.1016/j.ypmed.2020.106263 |
- Hospitals: work off a budget (profit) model; administrators make short term decisions, rather than long-term vision and goals. PPE is not charged/billed to patients or insurance companies. It is simply a cost to hospitals. Therefore they have no motivation to have updated stockpile.
- Demand shock: common during pandemics, leading to hoarding affected PPE, increased cost
- Government: Trump admin in trade war with China, slow to enact defense production act, federal stockpile inadequate (3 million masks, if 30% of population sick we would have needed 3.5 billion masks). Noted, expired federal stockpile, not restocked by prior administrations
- Supply Chain: US is an exporter of health goods, importer of goods from China. Cost 6x Nn5, gowns doubled cost
- Medical schools continue teach racial inferiority theories-- leading to inequitable management of HF, kidney disease, VBAC. For more information, see this NEJM paper.
- There is the widely-known Tuskegee Syphilis study and its repercussions, where respected clinicians and scientists intentionally harmed black bodies.
- Pediatric ED study from 2019, in which providers less likely to order tests/admissions for Latinx and Black children
- And widely held beliefs amongst medical students and resident trainees measured in 2016 that black people literally have thicker skin than white people and therefore feel less pain.

Global Inequity


But, Dr. Carmen points us, COVID feels more like this. Like we might never get to the wiser living phase and are maybe stuck in the disillusionment phase forever. . .

So, says Dr. Carmen, the hero narrative isn't enough. It leaves us feeling let down because it
- fails to address limitations of budget centered hospital model
- is a poor reflection of government inaction
- removes a sense of reciprocity and their responsibility during a global crisis
- centers discussions of racial inequality on individual patients and not institutional change
- did not protect our public health initiatives
- only superficially addresses the mental health efforts of providers

- Logos: dissect our fact to convince our audience
- public health over profit: with regards to PPE, remove profit motive. Strengthen local and state government to have stockpiles, Change industry policy to less foreign alliance, innovative/reusable PPE. Increase physician training pipelines. Change the way we deliver healthcare (e.g. concierge for safety net, wraparound services), explore models of innovative healthcare
- Ethos: build on ethics, sense of credibility.
- Address racism in medicine. Redesign curriculum to eliminate race-based science, support physicians of color, all healthcare workers of color. Support public health initiatives that use community-based participatory tools to target racial inequality (e.g. Promotora models)
- Pathos: being vulnerable with our emotions.
- Work collectively to build resilience. Support unionized healthcare workers who are most vulnerable (RNs, EVS, resident physicians), build a stronger telemedicine curriculum, normalize time to access mental health resources (encourage healthcare workers to go to those mental health visits), pay appropriately for work/hazard we have experienced. CA AB650 Retention Bonus (hazard pay), and more.



No comments:
Post a Comment