
Many, many thanks to Dr. Guille Freschl, who gave Grand Rounds this week titled Understanding Methamphetamine Use Disorder: A Deep Dive. This was our first R3 Grand Rounds Presentation of the academic year, and Dr. Freschl knocked it out of the park. The link to a video recording of her presentation is available here. Below find my notes.
A recording of this presentation can be viewed HERE.
***
Dr. Freschl was motivated to present on this topic by a longstanding interest in substance use disorders coupled with curiosity and concern about the oft uttered "Oh, it's probably because of the meth" that she heard from the mouths of her teachers. She was left wondering where the science meets the bias.
Did you know that amphetamine-type stimulants are the most widely used drugs in the world after cannabis? Did you know that between 2011 and 2016, overdoses from methamphetamine TRIPLED and that 1/4 of all overdoses in 2021 in the US were due to meth?
Methamphetamine use disorder can be seen all over the nation, but prevalence varies per region. Rates are highest in the West Coast and South. For example, prevalence of reported meth use in the past year in CA is reported at 1.04% of all adults, almost twice as much as most states in the Northeast (see map below).

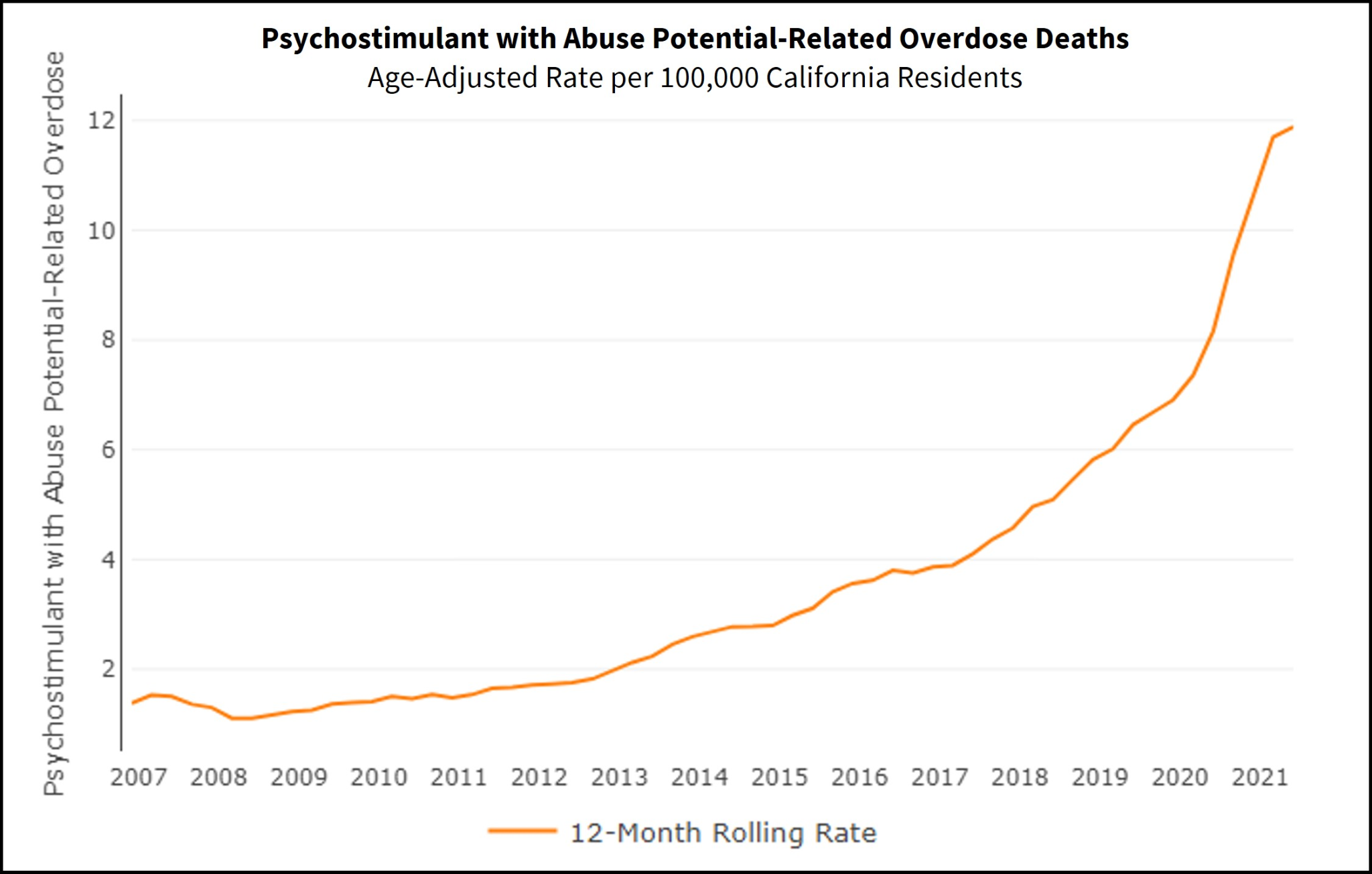
In California, non-fatal ED visits and overdose deaths have both risen over the last decade. In fact 32% of those in court-mandated substance use disorder treatment programs were there due to methamphetamine use. While the bulk of media and political attention is currently focused on opiates, one wonders, why aren't we talking more publically about methamphetamine?

What is methamphetamine?
Methamphetamine is an amphetamine derivative, notable for its additional methyl group; it enhances dopamine and norepinephrine in the synaptic cleft. Meth has a very long half life (12 hours cmpared to 90 minutes for cocaine).

Why is meth bad? So many reasons. . . keep reading to understand a few of the major adverse effects.
Cardiovascular toxicity
CV toxicity is the #1 cause of death in patients using methamphetamines, and risk of sudden cardiac death is increased by 27% with active meth use. CV toxicity includes a range of end-organ issues, including:
1) Hemorrhagic and ischemic strokes, due to vasoconstrictive effects and cerebral hypoperfusion
2) Very high rates of coronary artery disease (CAD) -- half of patients with regular meth use have CAD, despite lower rates of obesity and diabetes in these patients. This is thought to be directly related to the pro-inflammatory effects of meth.
3) Angina, which does not respond well to nitroglycerin, is common, due to vasospasm
4) Pulmonary hypertension, especially with IV meth use, due to damage to pulmonary endothelial cells
5) Severe systolic dysfunction with LV dysfunction is another sequalae of meth use
6) Ventricular arrhythmias are notable
Neurotoxicity
Neurotoxicity is the #2 cause of morbidity and mortality in patients using meth. It rapidly crosses the blood brain barrier. It does a doozy on the brain, including disrupting pleasure centers, creating episodic memory issues, damaging executive function (2/3 of people with regular meth use show cognitive impairment, worse with older age and longer duration and frequency of use), disrupting motor function (including fine motor and choreas), and can lead to psychosis similar to schizophrenia (delusions of persecution, auditory hallucinations, and formication in almost half of people using).
There is also a direct relationship between meth use and Parkinson's disease.
Dental effects
Serious dental effects include caries, tooth loss, tooth fractures -- all due to decreased saliva production (xerostomia), teeth grinding and jaw clenching that occurs with meth use.

Medication Assisted Therapy (MAT)?
Unfortunately, there are no FDA approved treatments for methamphetamine use disorder. A large meta-analysis of 43 RCTs with over 4000 patients found no clear evidence-based effective treatment.
These included trials with mirtazapine (conflicting results), methylphenidate, bupropion, naltrexone and modafinil (limited evidence of benefit, no support for routine use). In addition, anticonvulsants, antidepressants, antipsychotics all low strength and insufficient evidence. Bummer.
There was a small study that suggests that methylphenidate may be associated with decreased use over time: no difference at 30 days, but decreased in self reported use days at 10 weeks.
Also, a small study of combination therapy -- IM naltrexone (380mg q3 weeks) PLUS PO bupropion (450mg daily) small treatment effect of 11% reduction in meth use.
Hopefully, people will continue to investigate different agents for MAT and treatment of meth use disorder!
In conclusion, Dr. Freschl recommended that we use shared decision-making with patients when talking about trialing non-FDA approved treatment options. She reminded us to screen for CV and neurological sequelae of methamphetamine use.


No comments:
Post a Comment