
A recording of this presentation can be viewed HERE.
***
Thank you to local SMGR Oncologist, Dr. Zeyad Kanaan, for an action-packed presentation this week on Oncologic Emergencies. His presentation focused on five major emergencies-- SVC syndrome, Tumor Lysis syndrome, Hypercalcemia of malignancy, Acute malignant cord compression, and Leukostasis. Sprinkled among the five oncologic emergencies was a necklace of pearls for the primary care provider caring for cancer patients.
Here are a few general pearls:
- Primary care providers diagnose cancers; oncologists treat them.
- Oncologists cannot begin treatment of any cancer without a biopsy (i.e. "tissue is the issue")
- It can be anxiety-producing to carry a patient through the process of a cancer discovery and arranging the appropriate plan for biopsy.
- Oncologists can help guide us through this part, even if they are not yet managing the cancer.
- All cancer symptoms (e.g. chemo-related nausea and vomiting) are graded 0-5 (1 is mild, 5 is most severe).
- Most people with Gr 1 &2 symptoms can be managed as outpatient.
- Patients with Grade 3 sx should be sent to the ER.
- Gr 4 is life-threatening (often means ICU).
- Aggressive cancers, by definition, replicate and grow rapidly, which means they also tend to respond quickly to treatments.
- BUT aggressive cancers can also can come back quickly
- All oncologic emergencies require an urgent management plan, a plan for the next few days (less urgent).
- Ultimate management is treatment of the underlying cancer.
SVC Syndrome
SVC syndrome is caused by obstruction of the SVC, leading to facial edema and sometimes arm edema. The most common cause of SVC syndrome is cancer (particularly lung cancer, lymphoma, germ cell tumors). But there are other less common things that can obstruct the SVC.

Medial and perihilar masses are more likely to be squamous cell cancer and small cell lung cancers.
If you see "central necrosis" on imaging it means that the cancer is very aggressive and is growing too fast for its own blood supply.
As mentioned above, SVC Syndrome is graded 0-5. Grade 3 symptoms require ER/hospital management and definitive treatment of the underlying cancer, which means urgent initiation of chemotherapy.
Grade 4 requires a stent (rarely done).
SVC syndrome, regardless of Grade, is a bad prognostic sign.
Tumor Lysis Syndrome (TLS)
TLS is an oncologic emergency caused by massive tumor cell lysis with the release of large amounts of potassium, phosphate, and nucleic acids into the systemic circulation. TLS is more common in solid tumors. TLS can lead to AKI, cardiac arrythmias and even seizures. TLS can be diagnosed either clinically or via lab tests (lab abnormalities: hyperkalemia, hyperphosphatemia, hypocalcemia, and hyperuricemia). TLS can occur spontaneously with aggressive cancers and/or can also occur with initiation of chemotherapy.

Treatment of TLS:
1) Aggressive Hydration (1-2L bolus, followed by 200-300ml/hr crystalloids)
2) Urine alkalization (via bicarbonate drip)
3) Allopurinol -- allopurinol is a preventive drug for TLS, does nothing to an already elevated uric acid and cannot help urgently. Given PO. Dosed 100mg/m2 or 10mg/kg/day (divided q8h). Often started in solid tumors prior to chemo initiation. Dose needs to be reduced by 50% with renal failure.
4) Rasburicase -- considered a rescue agent, very potent cleavage of uric acid, $$$, very effective within 30 minutes. Usually requires only one dose (3mg, which is half of the manufacturer recommended dose), check uric acid daily. Can repeat but hardly ever necessary.
Both allopurinol and rasburicase should be started together in cases of TLS. Of note, both allopurinol and rasburicase can (and should) be given prophylactically in cases where TLS is highly anticipated.
Hypercalcemia of Malignancy
"moans, bones, and psychic overtones"
Lytic cancers that metastasize to bone are most likely to cause hypercalcemia. These include, most commonly breast cancer, multiple myeloma, lymphomas, and leukemias. Prostate cancer, e.g. while often spreading to bones, is less likely to be lytic.
1) Aggressive hydration
2) Bisphosphonates (+Denosumab) take a little longer than calcitonin. Works in ~2 days.
3) Calcitonin: is the acute treatment of choice, will drop the calcium quickly, but Ca will rise again quickly if otherwise left untreated
Once Ca starts dropping, goal is to treat the underlying cause.
Don't forget to check labs to be sure it's hypercalcemia of malignancy. A low intact PTH and elevated PTHrP is most consistent with malignant hypercalcemia. HyperCa in setting of elevated vitamin D levels, more often seen in lymphoma, is more likely to respond to steroids.
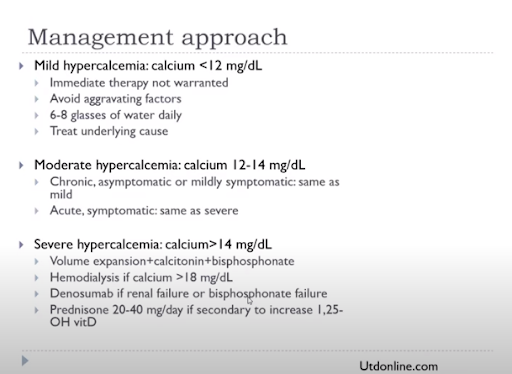
Mild hyper Ca (<12): oral hydration, treat the underlying cause
Mod hyper Ca (12-14): need IV hydration
Severe hyper Ca (>14): IVF, calcitonin, bisphosphonates, Hemodialysis can be helpful if Ca>18, desnosumab if renal failure. prednisone if elevated Vitamin D
In the end, once again you must treat the underlying cause.

Acute Malignant Cord Compression
This is a true oncologic emergency.
The thoracic vertebrae is the most common spinal place for cancer to go (lumber spine is the next most common). The cancer spot may actually be very small, but it is the edema leading to the cord compression and symptoms of pain and weakness. A patient's pre-intervention neurologic status influences a patient's chance of regaining function
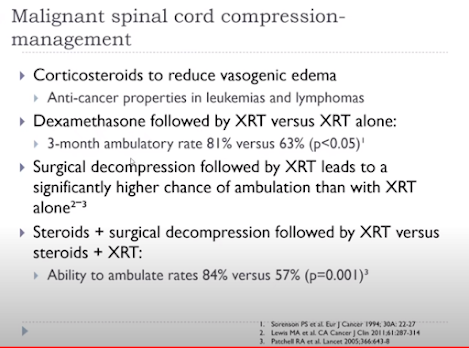
Hours can matter in terms of neurological preservation, so do not be afraid to start steroids. Primary care and ED's job is to 1) start steroids -- dexamethasone 4mg q6 hours (total 16 mg/day) and 2) call the neurosurgeon.
The vasogenic edema will respond quickly to the steroids.
Leukostasis = hyperviscosity (of Waldenstrom)
Most common symptoms: bleeding, blurred vision, headache, vertigo
Treatment is IVF to decrease viscosity
Check serum viscosity (>4 is significant)
Check IgM level
Plasmapheresis is very effective
Local patients with acute leukemia are admitted for urgent chemo (either to Alta Bates or Sacramento)
Goal is to treat leukostasis (WBC<100K), end organ effects (e.g. CAD) and leukemia all at once
Goal is to treat leukostasis (WBC<100K), end organ effects (e.g. CAD) and leukemia all at once



No comments:
Post a Comment