
A recording of this presentation is available HERE.
***
Many thanks to senior resident, Dr. Rebecca Walton, for a thought-provoking Grand Rounds presentation this week on Functional Disorders. Such an important and challenging topic!
What are functional disorders, you ask? As the name implies, functional disorders is not one entity; it is an umbrella term for a group of syndromes including functional GI disorders (e.g. IBS), fibromyalgia, interstitial cystitis, chronic pelvic pain, chronic headaches, and chronic fatigue.
Functional disorders are all disorders that do not have an identifiable disease label (at least not in our world of allopathic medicine) and feature "normal labs" but negatively impact the functioning of the body. They tend to be chronic and some are relapsing.
Functional disorders can be challenging to treat, cause patients and providers frustration and distress, and are steeped in bias. Functional disorders have their roots in psychiatric disorders: Freud's conversion disorder, substitution of a somatic symptoms for a mental one; hysteria, medically unexplained symptoms in multiple organ systems, often tied to the presence of a uterus; and somatic symptom disorder, a significant focus on physical symptoms that results in major distress or problems functioning.
Functional disorders are common in primary care and impose an impressive healthcare burden:
- Functional GI disorders represent 12% of the workload in primary care and 30% of outpatient GI consultations
- Fibromyalgia affects 2-4% of the population, and can lead to up to 10 outpatient visits per person per year
- Chronic headaches, one of the most common complains for neurological referral, are found in 4-5% of the population and results in, on average, 9 days of missed work per year
- no objective tissue or laboratory findings
- a genetic and/or environmental predisposition
- stress as triggering or exacerbating symptoms
- dysfunctional pain or sensory processing
- do not respond to therapies used for pain (e.g. acetaminophen)

Those who are already facing healthcare discrimination are prone to having functional disorders and thus experience further neglect
There is ongoing research into these syndromes, and I hope that soon the “lack of biomedical markers” changes
Even without biomedical markers, these symptoms matter
https://pubmed.ncbi.nlm.nih.gov/32294476/
https://www.sciencedirect.com/science/article/abs/pii/S0049017222001111?via%3Dihub
https://www.sciencedirect.com/science/article/abs/pii/S0049017207001473?via%3Dihub
https://pubmed.ncbi.nlm.nih.gov/22180058/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10507713/



This comment has been removed by the author.
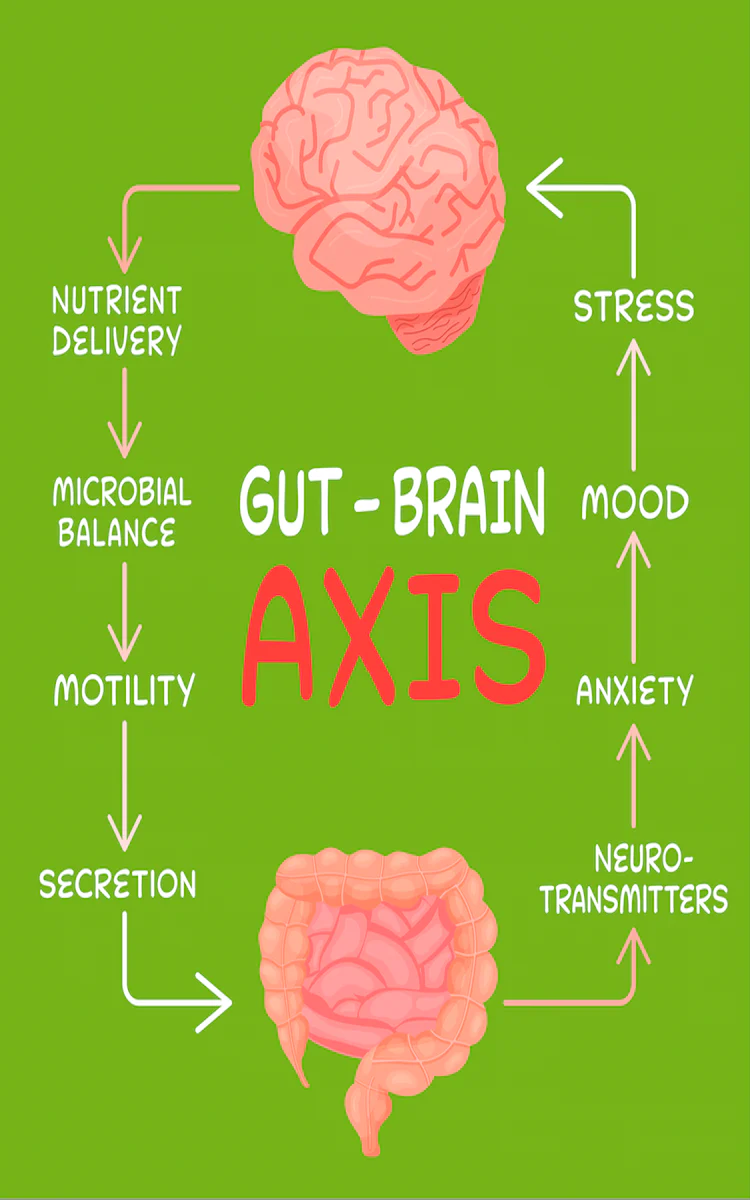
ReplyDeleteDr. Walton’s insights on the HPA axis and gut microbiome are fascinating. Dealing with 'normal labs' while suffering is incredibly frustrating. It highlights why finding a functional medicine doctor near me is so vital for addressing these complex, invisible symptoms holistically.
ReplyDelete