
A recording of this presentation is available HERE.
***
Many thanks to Dr. Briga Mullin for an excellent presentation this week on Prenatal Genetic Testing. Dr. Mullin reminded us from the get go -- that all patients have the right to accept or decline testing after counseling. Then she proceeded to update us on current prenatal genetic screening recommendations available to prenatal care providers and to pregnant patients.
This topic is ever-changing, as genetic screening tools become increasingly sophisticated. If you want to watch the entire presentation, please see the link above. Here are my notes.
It is important to make the distinction for patients and ourselves between SCREENING and DIAGNOSTIC tests. As we know, screening tests are those designed to "pick up" disease in patients who are otherwise well-appearing; in the case of prenatal genetic screening, they are designed to assess a pregnancy for the risk of certain congenital conditions. Diagnostic tests are designed to confirm a specific diagnosis.
In the world of prenatal genetic testing, current screening tests available to pregnant patients include: carriers testing, cell free DNA (cfDNA), AFP, early 1st tri and 2nd trimester ultrasound. The two currently available prenatal diagnostic tests are chorionic villous sampling -- CVS-- (10-13 weeks) and amniocentesis (>15 weeks).
 |
Carrier Screening
Carrier screening looks for autosomal recessive and x-linked conditions in maternal DNA. There is a huge range of options for carrier testing -- patients can be tested for up to 400 conditions, depending on the assay. ACOG currently recommends universal carrier screening for three conditions: 1) spinal muscular atrophy (SMA), 2) cystic fibrosis (CF), and 3) hemoglobinopathies. ACOG additionally recommends carrier screening for specific populations: Fragile X if a family history of intellectual disabilities and Tay Sachs disease for people who identify as Ashkenazi Jews, French Canadians and people of Cajun descent.
Sutter/CPMC currently offers a 112 gene expanded carrier screening panel (called "Horizon" by Natera). In contrast, SRCH -- via Quest labs -- offers a 3-condition carrier panel, which includes CF, Fragile X and SMA.
Of note, it is only necessary to screen maternal serum once in a lifetime, ideally before pregnancy. If a patient screens positive for any of these conditions, the partner should be offered carrier testing as a follow-up. If BOTH parents screen positive, diagnostic testing via CVS, amniocentesis or even IVF with embryo testing are options.
Cell Free DNA (cfDNA)
cfDNA tests look for placental DNA in maternal serum. Typically, cfDNA screens for three trisomies - Trisomy 18 (Edwards Syndrome), 21 (Down Syndrome) and 13 (Patau Syndrome). cfDNA is 98% sensitive in detecting these three trisomies. The gender of the fetus can also be identified with cfDNA. Testing is ideally done after 9-10 weeks gestational age because enough placental DNA is present at this time in the maternal serum to reliably detect and test. Of note, placental mosaicism does exist and can lead to a false positive screening test with cfDNA.
The California Genetic Disease Screening Program (GDSP) currently offers statewide cfDNA through their prenatal screen program to all patients with Medi-Cal. Their test detects Trisomy 18, 21, and 13 and gives gender as well. As of 4/1/2024, the GDSP program will also test for chromosomal aneuploidies.
Natera's Panorama screen, available to some privately insured patients, screens for for additional conditions. These tests cost between $170 and $300 out of pocket if not covered by insurance.
Early Anatomy Ultrasound (previously called nuchal translucency or NT ultrasound)
This ultrasound is generally performed at 10-13 weeks and is offered to detect severe structural anomalies (e.g. anencephaly). Given that it is only 70% sensitive for Down Syndrome, NT should no longer be used for screening over cfDNA. Arguments for doing an early anatomy ultrasound is to allow women to be able to terminate a pregnancy with severe structural anomalies as early as possible.
Maternal Serum Alpha Feto Protein (MSAFP)
For many of us in practice, this OG of prenatal genetic screening tests. It is a maternal serum test done between 15-20 weeks EGA and still has utility in the detection of neural tube defects (e.g. spina bifida) and abdominal wall defects (e.g. omphalocele and gastroschisis). Recommendations are evolving but it does screen for defects that are not otherwise picked up on cfDNA and can be done prior to a second trimester ultrasound, and so some guidelines encourage using it in addition to cfDNA for this reason, particularly for higher risk patients (e.g. family history, maternal age, etc).
Second Trimester Ultrasound (Anatomy survey)
This is another screening tool that has a decently long history -- usually an ultrasound performed between 17-21 weeks EGA to look at the fetal anatomy. In actuality, there are two versions of this ultrasound: the original Level 1 ultrasound, performed by a radiology tech with static images interpreted by a radiologist and Level 2 ultrasound, performed by a maternal-fetal-medicine (MFM) physician. Level 1 ultrasounds have historically been considered adequate for "low risk" pregnancies, but local practice has evolved such that most pregnant women in Santa Rosa are offered a Level 2 ultrasound as the screening test of choice. This is, of note, not a current ACOG recommendation. Some argue that Level 2 ultrasounds have less false positive findings because of the skill of the technician performing the study.
***
Regardless of which modality of prenatal genetic screening you are discussing with patients, the concept of shared decision-making is absolutely central to the practice of prenatal care. Shared decision making with pregnant patients should be 1) clear 2) objective and 3) non-directive. This can be challenging at times and take time to elicit a patient's values and goals as part of this discussion.
There are patients for whom knowledge will absolutely change the way they experience their pregnancy. Some who might terminate or choose to deliver in a different setting based on the findings. There are others for whom the anxiety of choosing a screening modality that could return a false positive result is not worth it. See the slide image below to consider ways in which shared decision making can be considered for different types of patients.

Remember that a positive screening test is not the same as a positive diagnostic test. The follow-up for most positive prenatal screens is either a CVS or amniocentesis.
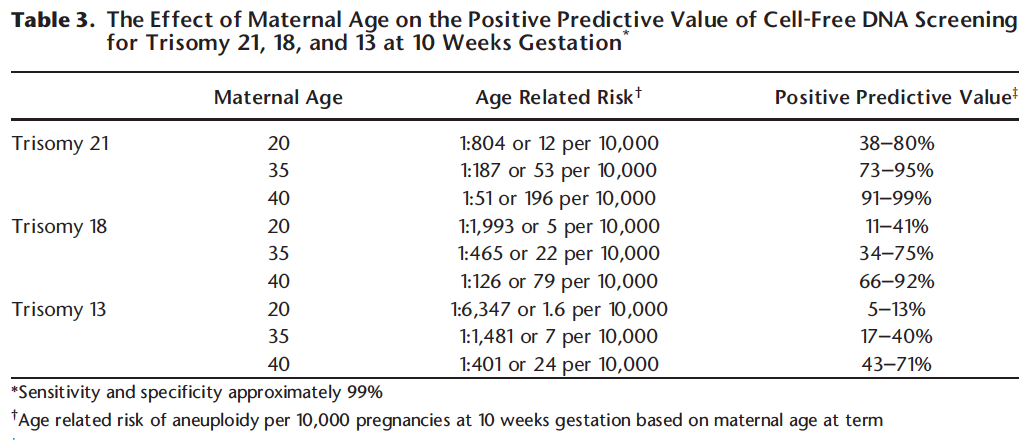
Positive Predictive Value
Also remember that positive predictive value of any test depends on the prevalence of that disease in the population, and in pregnancy, this is extremely dependent on maternal age. So, a positive cfDNA in a 40 year pregnant patient has very different implications than a positive cfDNA in a 20 year old patient. Dr. Mullin recommends the use of the prenatal screen calculator to help you help your patients understand their positive screening test.





No comments:
Post a Comment