The link for the recording of this session is HERE.
***
Many thanks to Dr. Suegee Tamar-Mattis and Celeste Monette, LCSW for a really interesting Grand Rounds this week on the use of Ketamine Assisted Psychotherapy. Those of us in primary care know too well that our tools for managing mental illness -- treatment-resistant depression, suicidality, and PTSD, for example -- are terribly limited. Dr. Tamar-Mattis encouraged us to consider psychedelics as a powerful and increasingly evidence-based tool that may change patients' brains and lives. The use of psychedelics for mental health is not new, but it is quickly evolving. It strikes me that was once considered "fringe" is now moving into the mainstream.
As someone who has been practicing for over 15 years, one's willingness to take on something new is such an interesting concept in medicine. Are you an early adopter? Or do you wait for the evidence to be convincing? Do you feel comfortable with experimentation? Or do you prefer engaging only in the "standard of care"? Why? Why not?
My notes:
Dr. Tamar-Mattis opened their presentation with the new hope of psychedelic medicine -- this is not just prescribing medications, but the combination of psychedelics and therapy. That is, the use of ketamine to offer patients a novel window into their mental health that then allows them to engage in therapy in a productive way, thereby offering hope in an area that can otherwise feel hopeless.

Psychedelics have been shown to have impact on both neurogenesis and neuroplasticity in the brain, and it is their effects on neurons that may be key to why they work. In essence, psychedelics allows patients with deep neural pathways to rewire them and/or alter them by acting directly on the neuronal networks. This concept is often referred to as "the snow globe effect" -- that is, for many people with severe mental health issues, the neuronal pathways are fixed and, therefore, deeply carved in the metaphysical snow; thus, it is virtually impossible for patients to forge a new path. BUT, with the use of psychedelics, the snow globe (neuronal networks) is virtually "shaken up" and the fixed pathway is then uncarved, opening the possibility for patients to create a new pathway, a healthier one.
I love this concept for patients -- particularly for those who seem so stuck. And it is the very stuck patients that get most frustrated with us (providers and healthcare system) and are most frustrating to their clinicians.
***
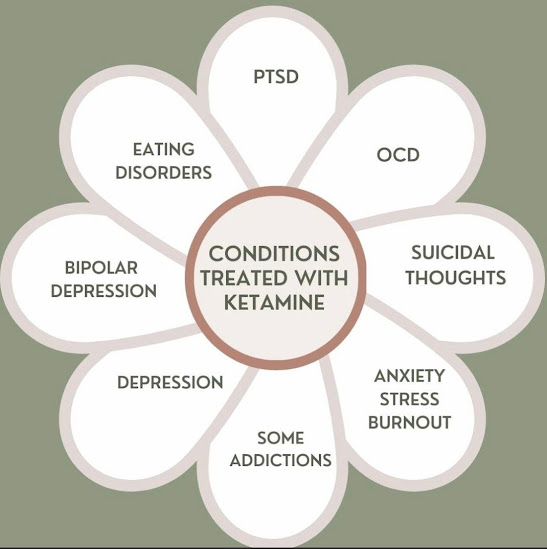
Ketamine is the only legal psychedelic at the federal level. There is evidence it works to improve mental health, even for patients who are already on SSRIs. It has a rapid anti-depressant effect and a rapid anti-suicidal effect. There is increasing evidence -- albeit small studies-- that it can positively impact PTSD, OCD, eating disorders, anxiety, some addiction, treatment-resistant depression and suicidality. In addition, there has been some use in developmental trauma and end of life issues.
For specific studies and data on the use of ketamine for psychiatric disease, see the reference list below**, which was compiled by Dr. Tamar Mattis.
Psychiatric contraindications: active mania in Bipolar I disorder, psychotic disorders, some personality disorders (particularly if very rigid or very unorganized)
Medical contraindications: heart disease (particularly recent MI or new CAD), uncontrolled hypertension, liver disease (ketamine is metabolized in the liver), pregnancy, increased intra-cranial pressure, and oxygen dependence (due to risk of respiratory depression).
Side effects: regularly elevates BP 10-20mm Hg, nausea and vomiting (can pre-treat with ondansetron), respiratory depression (rare at doses used for treatment).
***
Ketamine cannot be absorbed orally. But can be delivered via
- Lozenges/troches
- Nasal spray
- IV
- Injection (subcutaneous)

**
Grunebaum MF, Galfalvy HC, Choo TH, Keilp JG, Moitra VK, Parris MS, Marver JE, Burke AK, Milak MS, Sublette ME, Oquendo MA, Mann JJ. Ketamine for Rapid Reduction of Suicidal Thoughts in Major Depression: A Midazolam-Controlled Randomized Clinical Trial. Am J Psychiatry. April 1, 2018 https://pubmed.ncbi.nlm.nih.gov/29202655/
Ballard ED, Yarrington JS, Farmer CA, Richards E, Machado-Vieira R, Kadriu B, Niciu MJ, Yuan P, Park L, Zarate CA Jr. Characterizing the course of suicidal ideation response to ketamine. J Affect Disord. December 1, 2018 https://pubmed.ncbi.nlm.nih.gov/30099268/
McInnes, L. A., Qian, J. J., Gargeya, R. S., DeBattista, C; Heifets, B. D. (2022, January 11). A retrospective analysis of ketamine intravenous therapy for depression in real-world care settings. Journal of Affective Disorders. Retrieved May 10, 2022, from https://www.sciencedirect.com/science/article/pii/S0165032721014142#sec0007
Witt K, Potts J, Hubers A, Grunebaum MF, Murrough JW, Loo C, Cipriani A, Hawton K. Ketamine for suicidal ideation in adults with psychiatric disorders: A systematic review and meta-analysis of treatment trials. Aust N Z J Psychiatry. May 14, 2020 https://pubmed.ncbi.nlm.nih.gov/31729893/
John G. Keilp, PhD; Sean P. Madden,; Julia E. Marver, PhD; Abigail Frawley, PhD; Ainsley K. Burke, PhD; Mohammad M. Herzallah, PhD Mark Gluck, PhD; J. John Mann, MD; and Michael F. Grunebaum: Effects of Ketamine Versus Midazolam on Neurocognition at 24 Hours in Depressed Patients With Suicidal Ideation. The Journal of Clinical Psychiatry. November 2, 2021.
https://www.psychiatrist.com/jcp/depression/ketamine-neurocognition-patients-with-suicidal-ideation/
The Effect of a Single Dose of Intravenous Ketamine on Suicidal Ideation: A Systematic Review and Individual Participant Data Meta-Analysis
Samuel T. Wilkinson, M.D., Elizabeth D. Ballard, Ph.D., Michael H. Bloch, M.D., M.S., Sanjay J. Mathew, M.D., James W. Murrough, M.D., Ph.D., Adriana Feder, M.D., Peter Sos, M.D., Ph.D., Gang Wang, M.D., Carlos A. Zarate Jr., M.D., Gerard Sanacora, M.D., Ph.D. Published Online:3 Oct 2017https://doi.org/10.1176/appi.ajp.2017.17040472
Jollant F, Colle R, Nguyen TML, et al. Ketamine and esketamine in suicidal thoughts and behaviors: a systematic review. Therapeutic Advances in Psychopharmacology. 2023;13. doi:10.1177/20451253231151327 https://journals.sagepub.com/doi/10.1177/0004867419883341
Anzolin AP, Goularte JF, Pinto JV, Belmonte-de-Abreu P, Cruz LN, Cordova VHS, Magalhaes LS, Rosa AR, Cereser KM, Kauer-Sant'Anna M. Ketamine study: Protocol for naturalistic prospective multicenter study on subcutaneous ketamine infusion in depressed patients with active suicidal ideation. Front Psychiatry. 2023 Mar 9;14:1147298. doi: 10.3389/fpsyt.2023.1147298. PMID: 36970275; PMCID: PMC10033666.
Ahmed GK, Elserogy YM, Elfadl GMA, Ghada Abdelsalam K, Ali MA. Antidepressant and anti-suicidal effects of ketamine in treatment-resistant depression associated with psychiatric and personality comorbidities: A double-blind randomized trial. J Affect Disord. 2023 Mar 15;325:127-134. doi: 10.1016/j.jad.2023.01.005. Epub 2023 Jan 7. PMID: 36623562.
Chen, C. C., Zhou, N., Hu, N., Feng, J. G., & Wang, X. B. (2023). Acute Effects of Intravenous Sub-Anesthetic Doses of Ketamine and Intranasal Inhaled Esketamine on Suicidal Ideation: A Systematic Review and Meta-Analysis. Neuropsychiatric Disease and Treatment, 19, 587–599. https://doi.org/10.2147/NDT.S401032