
Many thanks to Dr. Allison Slater, our final resident from the class of 2024 to give her senior Grand Rounds presentation this week. She gave a really important and thought-provoking presentation on language and language interpretation in medicine. It was titled "To Understand and be Understood", a title she borrowed from a March 2017 AMA Journal of Ethics that focused on language, literacy and hierarchy in medicine.
A recording of her presentation can be found HERE.
My notes:
Dr. Slater began with a review of words:
- interpretation: spoken language being repeated in an alternate language
- translation: written language being repeated in an alternate language
The distinction between the two is important because trained interpreters have special training and skill in being able to perform live and capture the meaning of the discussion, whereas written translators have the tincture of time and the ability to be more precise. In the healthcare setting, we are generally using live interpretation with patients during patient encounters, though document translation is also important issue, particularly with regards to clinic after visit summaries and hospital discharge summaries.
- limited English proficiency (LEP): US Census distinction based on an individual's response to the question: "How well do you speak/read/write English". LEP is considered anyone who responds anything other than "very well"
- Non-English language preference: upon closer examination, the term LEP is a "deficit-oriented" distinction and in no way recognizes a person's proficiency in languages other than English. Thus, this may be the preferred term.
Professional interpretation in the healthcare setting is the law.
This legal protection comes through various acts and executive orders, but which has not always been accepted:
- 1964: Civil Rights Act codifies "national" origin as a protected class for all programs or activities receiving federal funds
- 2000: President Bill Clinton signs an executive order designed to improve access to services for patients with limited English proficiency (LEP) from all federally-funded agencies
- 2003: AMA president makes public statement that he sees "no need for professional interpreters"
- 2010: The Affordable Care Act (aka ACA/Obamacare) added protections for patients, including regulation around signage in 15 top languages for each state
- 2019: Trump rolls back and narrows protection
- April 26, 2024 (last week!): a federal appeals court reinstates the 2010 ACA protections that had been repealed in 2019
Despite the regulation requiring healthcare institutions to provide no-cost language interpretation for patients with non-English preference (and the real risk of malpractice vulnerability) we are al aware that what happens in real life is not always what should happen. Many healthcare providers "get by" with inadequate language skills, physicians in particular are well-documented to overestimate their language skills, and patients with LEP are known to have more adverse outcomes, longer hospital length of stay, have more tests, higher rates of readmission, and feel discriminated against in the places they are receiving health care.
Unfortunately, ad hoc or informal interpretation is often used -- including patient family members and/or non-trained staff. Ad-hoc interpreters -- i.e. anyone who isn't trained and certified-- introduce a range of possible challenges: the potential for role confusion, may not have adequate language abilities for the content, insufficient attention and recall, not following standard interpretation protocols, subjectivity and biased interpretation, breach of confidentiality, missed conversations, and the possibility of limited scope of inquiry (e.g. intimate sexual issues). In fact, one study found that 1/4 to 1/2 of questions asked by a clinician were misinterpreted or omitted by ad hoc interpreters
While "routine conversation" between LEP patients and clinicians who self-identify as being language proficient may be acceptable, clinicians should really be subject to a proficiency certification to ensure that vital medical conversations (e.g. diagnosis, surgery plans, medical treatment plans, procedural consents, and discharge plans) are correctly communicated. Medical communication requires precision -- and this is even more important with sensitive topics, e.g. mental health, options counseling, substance abuse, trauma, and sexual assault.
In addition, official interpreter roles can include exploration and explanation of culturally relevant features of a conversation.
Okay, deep breath. As I myself said at the end of her presentation, there are many ways in which much of what Dr. Slater shared has me feeling bad about myself. Even as someone who considers herself a champion for the best care for our patients with LEP, I often find myself acting badly: acting as an interpreter (myself without formal training), using family members for interpretation (twice in the last 2 weeks, interpreters in patient's preferred language were not readily available), failing to give an interpreter context, not ensuring that every person in the room has access to the same information.
Let's do better!
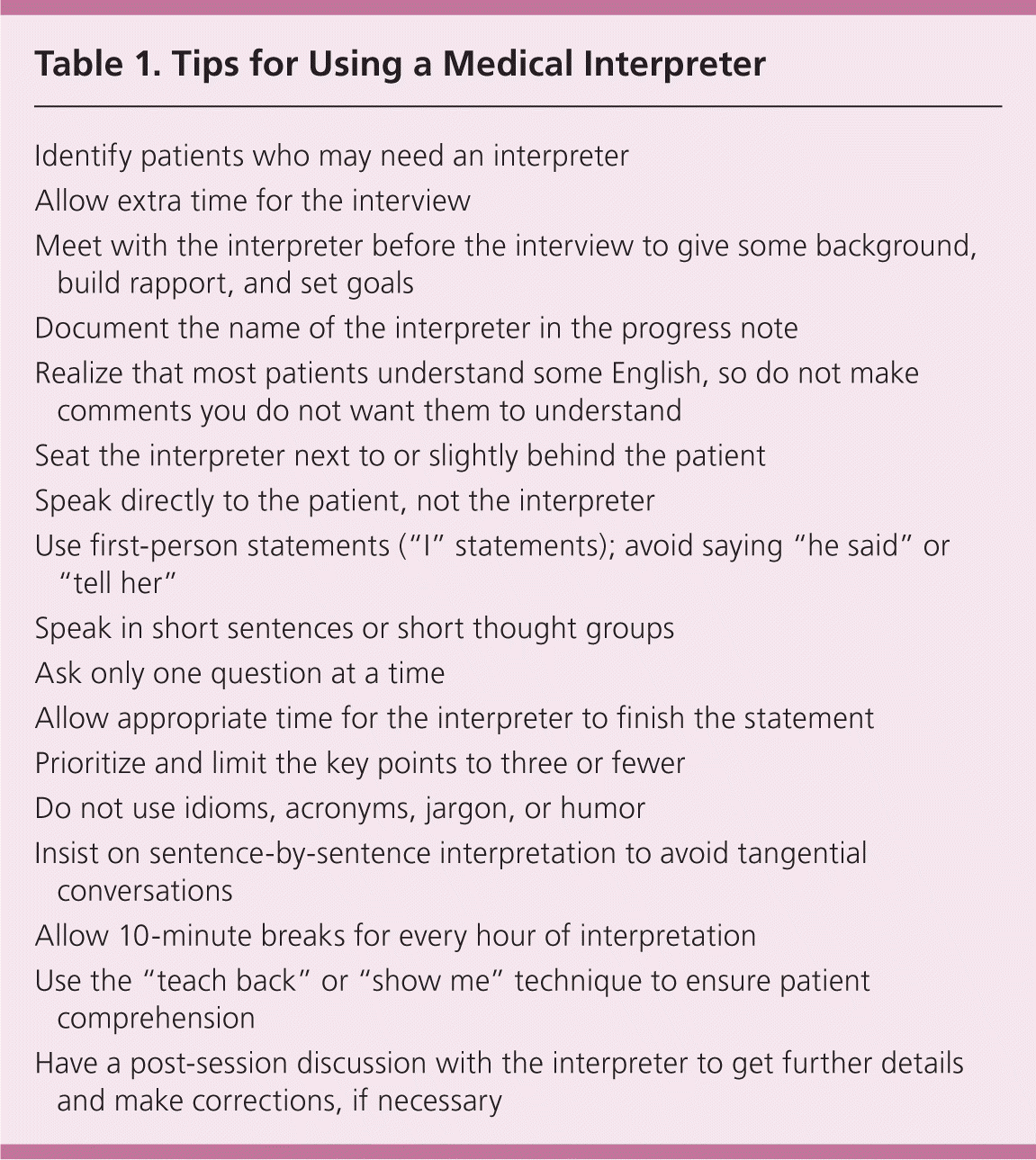
Best practices, my favorites: 1) Make sure you allow extra time 2) Always write down the ID# of the interpreter you are using 3) huddle with the interpreter before the conversation whenever possible 4) look for red flags (e.g. confusing answers, confusing questions, long statements that are not being appropriately interpreted) and 5) if you don't use an interpreter, document why. For more, see the Table below from the 2014 AAFP article, Appropriate Use of Medical Interpreters
Best practices, my favorites: 1) Make sure you allow extra time 2) Always write down the ID# of the interpreter you are using 3) huddle with the interpreter before the conversation whenever possible 4) look for red flags (e.g. confusing answers, confusing questions, long statements that are not being appropriately interpreted) and 5) if you don't use an interpreter, document why. For more, see the Table below from the 2014 AAFP article, Appropriate Use of Medical Interpreters



No comments:
Post a Comment