Many thanks to Dr. Janice Manjuck, our SSRRH ICU Director, for an excellent Grand Rounds this week on Oxygen Delivery and BiPAP for hospitalized patients. Dr. Manjuck gave us a nitty gritty review of when/how/why we might select one of many oxygen delivery devices. She combines humor, basic science, and evidence in just the right blend to bring us clinically relevant learning. We are so grateful!
A recording of her presentation is HERE. Feel free to check it out.
My notes:
First, off, when should we be using oxygen?

- if patient is acutely ill, oxygen is not indicated unless saturation is <96% (this excludes sickle cell crisis, CO poisoning, profound anemia (Hb <3) and pneumothorax
- in ACS/CAD aim for 93% saturation
Hypoxemia is a theoretical concern.
Pulse oximetry is not always reliable. SQ1 of 1 on the monitor tells us if the signal is reliable We should be suspicious about pulse oximetry -- it is not reliable in cases of poor perfusion, nail polish/artificial nails (think Olympic runners), tremor/movement disorder/seizure, anemia and CO poisoning (e.g. HB<5, bilirubin>30), bright lights (can falsely lower readings).
Of note, patients of color are MUCH less likely to have reliable reading from a pulse oximeter.
In a 2022 NEJM study of patients comparing ABG results to pulse oximeter readings, 11% of black patients had falsely elevated pulse ox readings (compared to 3% of white patients). This means a normal pulse oximeter reading may be falsely reassuring in BIPOC patients.
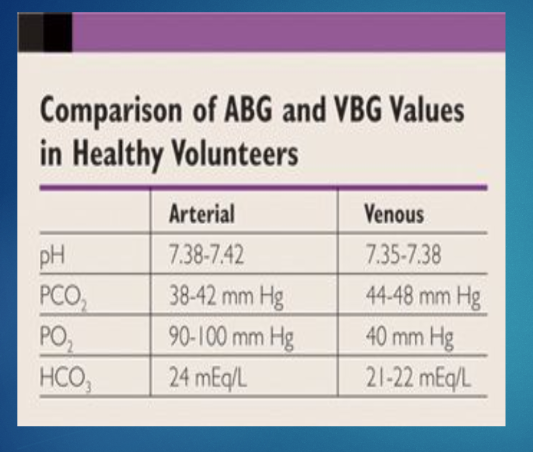
ABG vs. VBG: For patients NOT in shock, a VBG is a relatively good alternative to an ABG, particularly if you are getting the VBG to trend PCO2 in hypercapnic patients. VBGs are easier to get and less painful for patients. However, please note, if a patient is in shock, an ABG may be needed. Do not be offended if the intensivist asks for an ABG for an unstable floor patient!
Okay, when patients need oxygen, what kind of oxygen should I give them? It is important to take into account their clinical status, their comorbidities, and why they need oxygen. Low flow systems, which can deliver 0-15LPM of oxygen, are good for patients with a stable respiratory rate and pattern. High flow systems -- which can deliver 50-60 LPM-- may be better for patients who are more tachypneic.
Dr. Manjuck reviewed the concepts of anatomical dead space and entrainment
- Anatomical dead space is the internal volumes of the upper airways, in which no gas exchange takes place -- on average about 150 ML in a 70 kg person. Air is warmed, filtered and humidified in this space, but no gas exchange occurs. So it is essentially "wasted space".
- Entrainment is when room air mixes with oxygen due to a negative pressure gradient. In other words, it is the air that leaks around the oxygen delivery device. This is more common in nasal cannula<<face mask<<HFNC.
Which oxygen device is indicated? Depending on this oxygen needs of the patient, these two concepts may be important in which oxygen delivery device you choose. Other questions include: what interface is more desirable (e.g. nasal cannula vs. face mask)? how precise does the FiO2 need to be titrated? Does the air need to be humidified? Are other therapies (e.g. bronchodilator) needed? Low flow delivery tends to be more comfortable.
Low flow oxygen delivery systems include nasal cannula (NC), simple face mask, non-rebreather face mask, and venturi face masks. They can deliver 0-15 LPM of oxygen.
- Nasal cannula coming from wall is always delivering 100% oxygen, each 1L/min is equivalent to 3-4% FiO2, remembering that room air contains approximately 21% oxygen, SO
- 1 LPM=24% oxygen
- 2LPM=28% oxygen
- 3LPM=32% oxygen
- 4LPM=36% oxygen
- 5LPM=40% oxygen
- And so on. . .This means that 10 LPM on a nasal cannula gets you about 60% FiO2. See chart .

- A (simple) low flow mask can delivers upwards of 60-70% FiO2 IF the patient is breathing normally (essentially maxed out at 15LPM)
- A non-rebreather mask ALSO gives about 15LPM max of oxygen, which is ~60-70%. It does not flood the face, but rather floods the bag, which is a means to effectively deliver high levels of oxygen anywhere in the hospital. It can deliver 75-90% FiO2, but100% non-rebreather should be considered a fast track to something else (i.e. BiPAP, HFNC or intubation)
High flow systems include HFNC, CPAP, BiPAP, and mechanical ventilators; these are all positive-pressure systems and can deliver 15-60 LPM. This level of oxygen delievery is indicated in profound hypoxemia, hypercapnia AND/OR both.
Positive pressure systems can recruit alveoli, assist mechanical work of breathing, may ensure better oxygen delivery and increase functional residual capacity. Disadvantages include being confining/claustrophobia-inducing, may increase the need for sedation, increase risk of infection, increase in aerophagia, and they may reduce cardiac output (especially if patient is dry).
HFNC, which delivers 50-60 LPM, must ALWAYS be humidified and warmed. It offers "a little PEEP" for patients who need it. Good for elevated respiratory rate. Continuous high flow oxygen literally washes out the upper airways, leaving a reservoir of oxygen in the upper airway (pharynx) available for ongoing oxygen exchange. It also avoids rebreathing CO2, thereby decreasing anatomical dead space.
EPAP=CPAP=PEEP
Home CPAP has variable oxygen delivery, is not titratable, and not always humidified. Do NOT use home CPAP if patient hospitalized for respiratory reason. Hospital CPAP, on the other hand, is more titratable in terms of PEEP.
The worse the hypercapnia, the better to use BiPAP. Think of BiPAP as a non-invasive ventilator. It has different interfaces, can be humidified, you can titrate the oxygen more precisely, and you get feedback on its efficacy.









No comments:
Post a Comment