
A recording of this presentation is available HERE.
Many thanks to Dr. Andrew Brown, who gave an excellent Grand Rounds presentation this week on Integrative Approach to Anxiety and Depression. Anyone in primary care knows that we do a lot of management of psychiatric disorders in the primary care setting, often with very little specialty support. Many patients are interested in pursuing not just standard medical therapy (SSRI + cognitive behavioral therapy), but also integrative modalities.
Dr. Brown laid out the evidence for a wide range of non-pharmaceutical and non-psychotherapy treatments for anxiety and depression. The bottom line is that there are many, many, many integrative options with a range of small to moderate to strong evidence for the management of anxiety/depression. Put your seatbelts on. And don't use too many at once!
Integrative modalities, for the purpose of this talk include
- lifestyle/behavioral
- nutrition
- supplements and
- physical practices
Lifestyle/behavioral
Exercise works! The USPSTF recommends 2.5 hours/week of aerobic exercise for overall improved health. And good news, exercise can improved depression! Some exercise modalities may be better than others, including: include walking/jogging/yoga/strength training. The more "intense" the better. However, in a 2023 review article, ANY regular exercise, regardless of type, setting, or supervision decreased depression scores by 5-7 points.
There is not much evidence for exercise in anxiety, with a different review paper finding a benefit of exercise for anxiety in 7 of 25 studies and no benefit in the remaining 18.
It should come as no surprise that substance use and substance use disorders are frequent comorbidities with anxiety and depression. Note in the chart below:
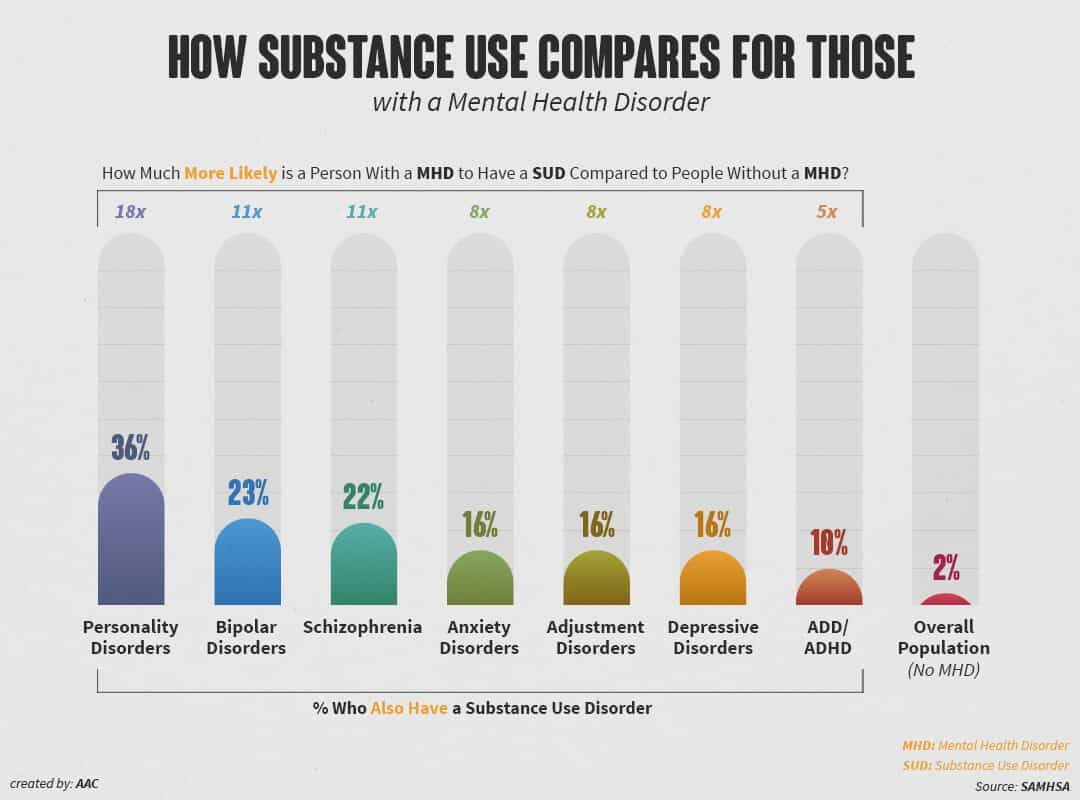
- 16% of people with anxiety disorder also have SUD
- 16% of people with an adjustment disorder also have SUD
- 16% of people with depression also have SUD

- Kava Kava (Piper methysticum): 50-70mg TID, mixed evidence, some concern for hepatoxicity
- St. John's Wort (Hypericum perforatum): strong evidence in depression, 500-1800mg/day. A 2017 Meta-analysis found it to be equivalent to SSRIs (of note, not safe to take at same time as SSRIs)
- Saffron (Crocus sativus): 30-200mg/day, strong evidence for depression and anxiety, $$ cost can be an issue, also concerns regarding first trimester SAB in early pregnancy
- Lavender (Lavandula angustifolia): "a few drops", moderate evidence, compared to lorazepam in a trial of preoperative patients was found to be "equivalent". SE: gynecomastia


- Vitamin D: stronger evidence in depression (than anxiety)
- B Complex, found in dark/green/leafy veggies, may be good adjunct
- Zinc: dose response benefit in depression and anxiety
- Magnesium: strong evidence as either monotherapy OR adjunct, depression more than anxiety, change of 4 points on GAD7 or PHQ9, so may be good choice for mild-mod depression/anxiety

- Acupuncture: 2024 Meta-analysis found that acupuncture was BETTER than SSRIs for depression, particularly if electro-acupuncture techniques are used. Most studies indicate that a combination of SSRI and acupuncture decreases rates of remission. There is less evidence for acupuncture in anxiety.
- Acupressure: no evidence for durable benefit, but may be good for episodic symptoms (and can be self-done)
- Progressive Muscle Relaxation: strong evidence in pre-procedural anxiety and symptoms report for patients. There are a wide range of muscle relaxation techniques, many can be taught in just a few minutes in the office setting
- Breathwork: Once again, there are many different breath practices. Two easy ones to teach in the office are: Box, 4-7-8 (see images below). Both have been shown to help with symptom management


de Noronha, S.I.S.R., de Moraes, L.A.G., Hassell, J.E. et al. High-fat diet, microbiome-gut-brain axis signaling, and anxiety-like behavior in male rats. Biol Res 57, 23 (2024). https://doi.org/10.1186/s40659-024-00505-1
Fatemi, F., Siassi, F., Qorbani, M. et al. Higher dietary fat quality is associated with lower anxiety score in women: a cross-sectional study. Ann Gen Psychiatry 19, 14 (2020). https://doi.org/10.1186/s12991-020-00264-9
Mohit Kumar, Babita Bhatt, Chitralekha Gusain, Nayan Mahajan, Mahendra Bishnoi, Sex-specific effects of ketogenic diet on anxiety-like behavior and neuroimmune response in C57Bl/6J mice, The Journal of Nutritional Biochemistry, Volume 127 (2024). https://doi.org/10.1016/j.jnutbio.2024.109591.
Haduch, A.; Bromek, E.; Kuban, W.; Daniel, W.A. The Engagement of Cytochrome P450 Enzymes in Tryptophan Metabolism. Metabolites 2023, 13, 629. https://doi.org/10.3390/metabo13050629
Gregory L. Stonerock, Rahul P. Gupta, James A. Blumenthal, Is exercise a viable therapy for anxiety? Systematic review of recent literature and critical analysis, Progress in Cardiovascular Diseases, Volume 83, 2024, Pages 97-115, https://doi.org/10.1016/j.pcad.2023.05.006.
Noetel M, Sanders T, Gallardo-Gómez D, Taylor P, del Pozo Cruz B, van den Hoek D et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials BMJ 2024; 384 :e075847 https://doi:10.1136/bmj-2023-075847
Kedzior, K.K., Laeber, L.T. A positive association between anxiety disorders and cannabis use or cannabis use disorders in the general population- a meta-analysis of 31 studies. BMC Psychiatry 14, 136 (2014). https://doi.org/10.1186/1471-244X-14-136
Berglund, M. and Ojehagen, A. (1998), The Influence of Alcohol Drinking and Alcohol Use Disorders on Psychiatric Disorders and Suicidal Behavior. Alcoholism: Clinical and Experimental Research, 22: 333s-345s. https://doi.org/10.1111/j.1530-0277.1998.tb04388.x
Lev-Ran S, Roerecke M, Le Foll B, George TP, McKenzie K, Rehm J. The association between cannabis use and depression: a systematic review and meta-analysis of longitudinal studies. Psychological Medicine. 2014;44(4):797-810. doi:10.1017/S0033291713001438
Pinto JV, Crippa JAS, Ceresér KM, Vianna-Sulzbach MF, Silveira Júnior ÉM, Santana da Rosa G, Testa da Silva MG, Hizo GH, Simão Medeiros L, Santana de Oliveira CE, Bristot G, Campos
AC, Guimarães FS, Hallak JEC, Zuardi AW, Yatham LN, Kapczinski F, Kauer-Sant'Anna M. Cannabidiol as an Adjunctive Treatment for Acute Bipolar Depression: A Pilot Study: Le cannabidiol comme traitement d'appoint de la dépression bipolaire aiguë : une étude pilote. Can J Psychiatry. 2024 Apr;69(4):242-251. doi: 10.1177/07067437231209650. Epub 2023 Nov 3. PMID: 37920963; PMCID: PMC10924581.
Gebara MA, Siripong N, DiNapoli EA, Maree RD, Germain A, Reynolds CF, Kasckow JW, Weiss PM, Karp JF. Effect of insomnia treatments on depression: A systematic review and meta-analysis. Depress Anxiety. 2018 Aug;35(8):717-731. doi: 10.1002/da.22776. Epub 2018 May 21. PMID: 29782076.
Fava M, Schaefer K, Huang H, Wilson A, Iosifescu DV, Mischoulon D, Wessel TC. A post hoc analysis of the effect of nightly administration of eszopiclone and a selective serotonin reuptake inhibitor in patients with insomnia and anxious depression. J Clin Psychiatry. 2011 Apr;72(4):473-9. doi: 10.4088/JCP.09m05131gry. Epub 2010 Nov 2. PMID: 21208574.
Nagy E, Moore S. Social interventions: An effective approach to reduce adult depression? J Affect Disord. 2017 Aug 15;218:131-152. doi: 10.1016/j.jad.2017.04.043. Epub 2017 Apr 24. PMID: 28472703.
Cruwys T, Alexander Haslam S, Dingle GA, Jetten J, Hornsey MJ, Desdemona Chong EM, Oei TP. Feeling connected again: interventions that increase social identification reduce depression symptoms in community and clinical settings. J Affect Disord. 2014 Apr;159:139-46. doi: 10.1016/j.jad.2014.02.019. Epub 2014 Feb 18. PMID: 24679402.
Beauchamp AM, Lehmann CU, Medford RJ, Hughes AE. The Association of a Geographically Wide Social Media Network on Depression: County-Level Ecological Analysis. J Med Internet Res. 2023 Mar 27;25:e43623. doi: 10.2196/43623. Erratum in: J Med Internet Res. 2023 Apr 11;25:e47896. doi: 10.2196/47896. PMID: 36972109; PMCID: PMC10131939.
Primack BA, Bisbey MA, Shensa A, Bowman ND, Karim SA, Knight JM, Sidani JE. The association between valence of social media experiences and depressive symptoms. Depress Anxiety. 2018 Aug;35(8):784-794. doi: 10.1002/da.22779. Epub 2018 Jun 6. PMID: 29877002.
Mizumoto T, Ikei H, Hagiwara K, Matsubara T, Higuchi F, Kobayashi M, Yamashina T, Sasaki J, Yamada N, Higuchi N, Haraga K, Kirihara F, Okabe E, Asai K, Hirotsu M, Chen C, Miyazaki Y, Nakagawa S. Mood and physiological effects of visual stimulation with images of the natural environment in individuals with depressive and anxiety disorders. J Affect Disord. 2024 Jul 1;356:257-266. doi: 10.1016/j.jad.2024.04.025. Epub 2024 Apr 7. PMID: 38588725.
Yeon PS, Jeon JY, Jung MS, Min GM, Kim GY, Han KM, Shin MJ, Jo SH, Kim JG, Shin WS. Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2021 Dec 1;18(23):12685. doi: 10.3390/ijerph182312685. PMID: 34886407; PMCID: PMC8657257.
https://medicine.umich.edu/sites/default/files/content/downloads/Relaxation-Skills-for-Anxiety.pdf
Heissel A, Heinen D, Brokmeier LL, Skarabis N, Kangas M, Vancampfort D, Stubbs B, Firth J, Ward PB, Rosenbaum S, Hallgren M, Schuch F. Exercise as medicine for depressive symptoms? A systematic review and meta-analysis with meta-regression. Br J Sports Med. 2023 Aug;57(16):1049-1057. doi: 10.1136/bjsports-2022-106282. Epub 2023 Feb 1. PMID: 36731907; PMCID: PMC10423472.
Gartlehner G, Dobrescu A, Chapman A, Toromanova A, Emprechtinger R, Persad E, Affengruber L, Pieh C, Klerings I, Wagner G. Nonpharmacologic and Pharmacologic Treatments of Adult Patients With Major Depressive Disorder: A Systematic Review and Network Meta-analysis for a Clinical Guideline by the American College of Physicians. Ann Intern Med. 2023 Feb;176(2):196-211. doi: 10.7326/M22-1845. Epub 2023 Jan 24. PMID: 36689750.
Sarris J, Marx W, Ashton MM, Ng CH, Galvao-Coelho N, Ayati Z, Zhang ZJ, Kasper S, Ravindran A, Harvey BH, Lopresti A, Mischoulon D, Amsterdam J, Yatham LN, Berk M. Plant-based Medicines (Phytoceuticals) in the Treatment of Psychiatric Disorders: A Meta-review of Meta-analyses of Randomized Controlled Trials: Les médicaments à base de plantes (phytoceutiques) dans le traitement des troubles psychiatriques: une méta-revue des méta-analyses d'essais randomisés contrôlés. Can J Psychiatry. 2021 Oct;66(10):849-862. doi: 10.1177/0706743720979917. Epub 2021 Feb 18. PMID: 33596697; PMCID: PMC8573706.
Jacobs B.P., Bent S., Tice J.A., Blackwell T., Cummings S.R. An internet-based randomized, placebo-controlled trial of kava and valerian for anxiety and insomnia. Medicine. 2005;84:197–207. doi: 10.1097/01.md.0000172299.72364.95.
Hausenblas H.A., Saha D., Dubyak P.J., Anton S.D. Saffron (Crocus sativus L.) and major depressive disorder: A meta-analysis of randomized clinical trials. J. Integr. Med. 2013;11:377–383. doi: 10.3736/jintegrmed2013056.
Lopresti A.L., Drummond P.D. Saffron (Crocus sativus) for depression: A systematic review of clinical trials and examination of underlying antidepressant mechanisms of action. Hum. Psychopharmacol. 2014;29:517–527. doi: 10.1002/hup.2434.
Kasper S., Gastpar M., Müller W.E., Volz H.P., Möller H.J., Schläfke S., Dienel A. Lavender oil preparation Silexan is effective in generalized anxiety disorder-A randomized, double-blind comparison to placebo and paroxetine. Int. J. Neuropsychopharmacol. 2014;17:859–869. doi: 10.1017/S1461145714000017.
Kasper S., Anghelescu I., Dienel A. Efficacy of orally administered Silexan in patients with anxiety-related restlessness and disturbed sleep—A randomized, placebo-controlled trial. Eur. Neuropsychopharmacol. 2015;25:1960–1967. doi: 10.1016/j.euroneuro.2015.07.024.
Kasper S., Volz H.P., Dienel A., Schläfke S. Efficacy of Silexan in mixed anxiety-depression-A randomized, placebo-controlled trial. Eur. Neuropsychopharmacol. 2016;26:331–340. doi: 10.1016/j.euroneuro.2015.12.002
Woelk H., Schläfke S. A multi-center, double-blind, randomised study of the Lavender oil preparation Silexan in comparison to Lorazepam for generalized anxiety disorder. Phytomedicine. 2010;17:94–99. doi: 10.1016/j.phymed.2009.10.006.
Janda K., Wojtkowska K., Jakubczyk K., Antoniewicz J., Skonieczna-żydecka K. Passiflora incarnata in Neuropsychiatric Disorders—A Systematic Review. Nutrients. 2020;12:3894. doi: 10.3390/nu12123894.
Sarris J, Kavanagh DJ, Byrne G, Bone KM, Adams J, Deed G. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of Piper methysticum. Psychopharmacology (Berl). 2009 Aug;205(3):399-407. doi: 10.1007/s00213-009-1549-9. Epub 2009 May 9. PMID: 19430766.
Liu RT, Walsh RFL, Sheehan AE. Prebiotics and probiotics for depression and anxiety: A systematic review and meta-analysis of controlled clinical trials. Neurosci Biobehav Rev. 2019 Jul;102:13-23. doi: 10.1016/j.neubiorev.2019.03.023. Epub 2019 Apr 17. PMID: 31004628; PMCID: PMC6584030.
Yang Y, Yang L, Wan M, Pan D, Sun G, Yang C. Assessment of optimal combinations of therapeutic probiotics for depression, anxiety, and stress. Psychol Med. 2024 Jul;54(10):2547-2561. doi: 10.1017/S0033291724000679. Epub 2024 Mar 18. PMID: 38497101.
Yosaee S, Clark CCT, Keshtkaran Z, Ashourpour M, Keshani P, Soltani S. Zinc in depression: From development to treatment: A comparative/ dose response meta-analysis of observational studies and randomized controlled trials. Gen Hosp Psychiatry. 2022 Jan-Feb;74:110-117. doi: 10.1016/j.genhosppsych.2020.08.001. Epub 2020 Aug 10. PMID: 32829928.
Ranjbar E, Kasaei MS, Mohammad-Shirazi M, Nasrollahzadeh J, Rashidkhani B, Shams J, Mostafavi SA, Mohammadi MR. Effects of zinc supplementation in patients with major depression: a randomized clinical trial. Iran J Psychiatry. 2013 Jun;8(2):73-9. PMID: 24130605; PMCID: PMC3796297.
Tarleton EK, Littenberg B, MacLean CD, Kennedy AG, Daley C. Role of magnesium supplementation in the treatment of depression: A randomized clinical trial. PLoS One. 2017 Jun 27;12(6):e0180067. doi: 10.1371/journal.pone.0180067. PMID: 28654669; PMCID: PMC5487054.
Wang H, Jin M, Xie M, Yang Y, Xue F, Li W, Zhang M, Li Z, Li X, Jia N, Liu Y, Cui X, Hu G, Dong L, Wang G, Yu Q. Protective role of antioxidant supplementation for depression and anxiety: A meta-analysis of randomized clinical trials. J Affect Disord. 2023 Feb 15;323:264-279. doi: 10.1016/j.jad.2022.11.072. Epub 2022 Nov 25. PMID: 36442656.
Borges-Vieira JG, Cardoso CKS. Efficacy of B-vitamins and vitamin D therapy in improving depressive and anxiety disorders: a systematic review of randomized controlled trials. Nutr Neurosci. 2023 Mar;26(3):187-207. doi: 10.1080/1028415X.2022.2031494. Epub 2022 Feb 14. PMID: 35156551.
Zhu C, Zhang Y, Wang T, Lin Y, Yu J, Xia Q, Zhu P, Zhu DM. Vitamin D supplementation improves anxiety but not depression symptoms in patients with vitamin D deficiency. Brain Behav. 2020 Nov;10(11):e01760. doi: 10.1002/brb3.1760. Epub 2020 Sep 18. PMID: 32945627; PMCID: PMC7667301.
Wang R, Xu F, Xia X, Xiong A, Dai D, Ling Y, Sun R, Qiu L, Ding Y, Xie Z. The effect of vitamin D supplementation on primary depression: A meta-analysis. J Affect Disord. 2024 Jan 1;344:653-661. doi: 10.1016/j.jad.2023.10.021. Epub 2023 Oct 16. PMID: 37852593.
Marschall J, Fejer G, Lempe P, Prochazkova L, Kuchar M, Hajkova K, van Elk M. Psilocybin microdosing does not affect emotion-related symptoms and processing: A preregistered field and lab-based study. J Psychopharmacol. 2022 Jan;36(1):97-113. doi: 10.1177/02698811211050556. Epub 2021 Dec 17. PMID: 34915762; PMCID: PMC8801668.
Tan Y, Duan R, Wen C. Efficacy of acupuncture for depression: a systematic review and meta-analysis. Front Neurosci. 2024 Apr 30;18:1347651. doi: 10.3389/fnins.2024.1347651. PMID: 38745939; PMCID: PMC11091333.
Zhichao H, Ching LW, Huijuan L, Liang Y, Zhiyu W, Weiyang H, Zhaoxiang B, Linda ZLD. A network meta-analysis on the effectiveness and safety of acupuncture in treating patients with major depressive disorder. Sci Rep. 2021 May 17;11(1):10384. doi: 10.1038/s41598-021-88263-y. PMID: 34001924; PMCID: PMC8129113.
Xu G, Lei H, Huang L, Xiao Q, Huang B, Zhou Z, Tian H, Huang F, Liu Y, Zhao L, Li X, Liang F. The dose-effect association between acupuncture sessions and its effects on major depressive disorder: A meta-regression of randomized controlled trials. J Affect Disord. 2022 Aug 1;310:318-327. doi: 10.1016/j.jad.2022.04.155. Epub 2022 May 2. PMID: 35504399.
Xu Z, Zhang X, Shi H, Liang M, Ning F, Wang Q, Jia H. Efficacy of acupuncture for anxiety and depression in functional dyspepsia: A systematic review and meta-analysis. PLoS One. 2024 Mar 7;19(3):e0298438. doi: 10.1371/journal.pone.0298438. PMID: 38452033; PMCID: PMC10919749.
Carlson LE, Ismaila N, Addington EL, Asher GN, Atreya C, Balneaves LG, Bradt J, Fuller-Shavel N, Goodman J, Hoffman CJ, Huston A, Mehta A, Paller CJ, Richardson K, Seely D, Siwik CJ, Temel JS, Rowland JH. Integrative Oncology Care of Symptoms of Anxiety and Depression in Adults With Cancer: Society for Integrative Oncology-ASCO Guideline. J Clin Oncol. 2023 Oct 1;41(28):4562-4591. doi: 10.1200/JCO.23.00857. Epub 2023 Aug 15. PMID: 37582238.
Fan JQ, Lu WJ, Tan WQ, Liu X, Wang YT, Wang NB, Zhuang LX. Effectiveness of Acupuncture for Anxiety Among Patients With Parkinson Disease: A Randomized Clinical Trial. JAMA Netw Open. 2022 Sep 1;5(9):e2232133. doi: 10.1001/jamanetworkopen.2022.32133. PMID: 36129711; PMCID: PMC9494193.
Wiles MD, Mamdani J, Pullman M, Andrzejowski JC. A randomised controlled trial examining the effect of acupuncture at the EX-HN3 (Yintang) point on pre-operative anxiety levels in neurosurgical patients. Anaesthesia. 2017 Mar;72(3):335-342. doi: 10.1111/anae.13785. Epub 2017 Jan 16. PMID: 28092106.
Molassiotis A, Suen L, Lai C, Chan B, Wat KHY, Tang J, To KL, Leung CO, Lee S, Lee P, Chien WT. The effectiveness of acupressure in the management of depressive symptoms and in improving quality of life in older people living in the community: a randomised sham-controlled trial. Aging Ment Health. 2020 Jun;24(6):1001-1009. doi: 10.1080/13607863.2019.1584789. Epub 2019 Mar 14. PMID: 30869991.
Linardon J, Messer M, Goldberg SB, Fuller-Tyszkiewicz M. The efficacy of mindfulness apps on symptoms of depression and anxiety: An updated meta-analysis of randomized controlled trials. Clin Psychol Rev. 2024 Feb;107:102370. doi: 10.1016/j.cpr.2023.102370. Epub 2023 Dec 3. PMID: 38056219; PMCID: PMC10872959.
Hofmann SG, Gómez AF. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr Clin North Am. 2017 Dec;40(4):739-749. doi: 10.1016/j.psc.2017.08.008. Epub 2017 Sep 18. PMID: 29080597; PMCID: PMC5679245.
Tan, Z.Y.A., Wong, S.H., Cheng, L.J. et al. Effectiveness of Mobile-Based Mindfulness Interventions in Improving Mindfulness Skills and Psychological Outcomes for Adults: a Systematic Review and Meta-regression. Mindfulness 13, 2379–2395 (2022). https://doi.org/10.1007/s12671-022-01962-z
Éva Gál, Simona Ștefan, Ioana A. Cristea, The efficacy of mindfulness meditation apps in enhancing users’ well-being and mental health related outcomes: a meta-analysis of randomized controlled trials, Journal of Affective Disorders, Volume 279, 2021, Pages 131-142, ISSN 0165-0327, https://doi.org/10.1016/j.jad.2020.09.134.
Goldberg, S. B., Lam, S. U., Britton, W. B., & Davidson, R. J. (2021). Prevalence of meditation-related adverse effects in a population-based sample in the United States. Psychotherapy Research, 32(3), 291–305. https://doi.org/10.1080/10503307.2021.1933646
Conrad A, Roth WT. Muscle relaxation therapy for anxiety disorders: it works but how? J Anxiety Disord. 2007;21(3):243-64. doi: 10.1016/j.janxdis.2006.08.001. Epub 2006 Sep 1. PMID: 16949248.
Jia Y, Wang X, Cheng Y. Relaxation Therapy for Depression: An Updated Meta-analysis. J Nerv Ment Dis. 2020 Apr;208(4):319-328. doi: 10.1097/NMD.0000000000001121. PMID: 32221187.
Köse Kabakcıoğlu N, Ayaz-Alkaya S. The effect of progressive muscle relaxation on stress, anxiety, and depression in adolescents: A quasi-experimental design. J Pediatr Nurs. 2024 Sep-Oct;78:89-96. doi: 10.1016/j.pedn.2024.06.014. Epub 2024 Jun 21. PMID: 38905787.




