
A recording of this presentation is available HERE.
Thanks to Dr. Ryley Saedi-Kwon for her presentation this week on Physiologic Birth. As usual, a recording of the presentation is available above. Dr. Saedi-Kwon covered a wide range of birth topics, see my highlights below.
Physiologic Birth, as outlined in a 2012 consensus statement of US midwifery organizations includes:
- Spontaneous onset and progression of labor
- Includes biological & psychological conditions that promote effective labor
- Results in the vaginal birth of the infant and placenta
- Results in physiological blood loss
- Facilitates optimal newborn transition through skin-to-skin contact
- Supports early initiation of breastfeeding
2018 systematic qualitative review found that
Most wanted a physiological labor and birth while acknowledging that birth can be unpredictable and frightening and they may need to ‘go with the flow’
Small minority birth was physical process that should be conducted as quickly and painlessly as possible
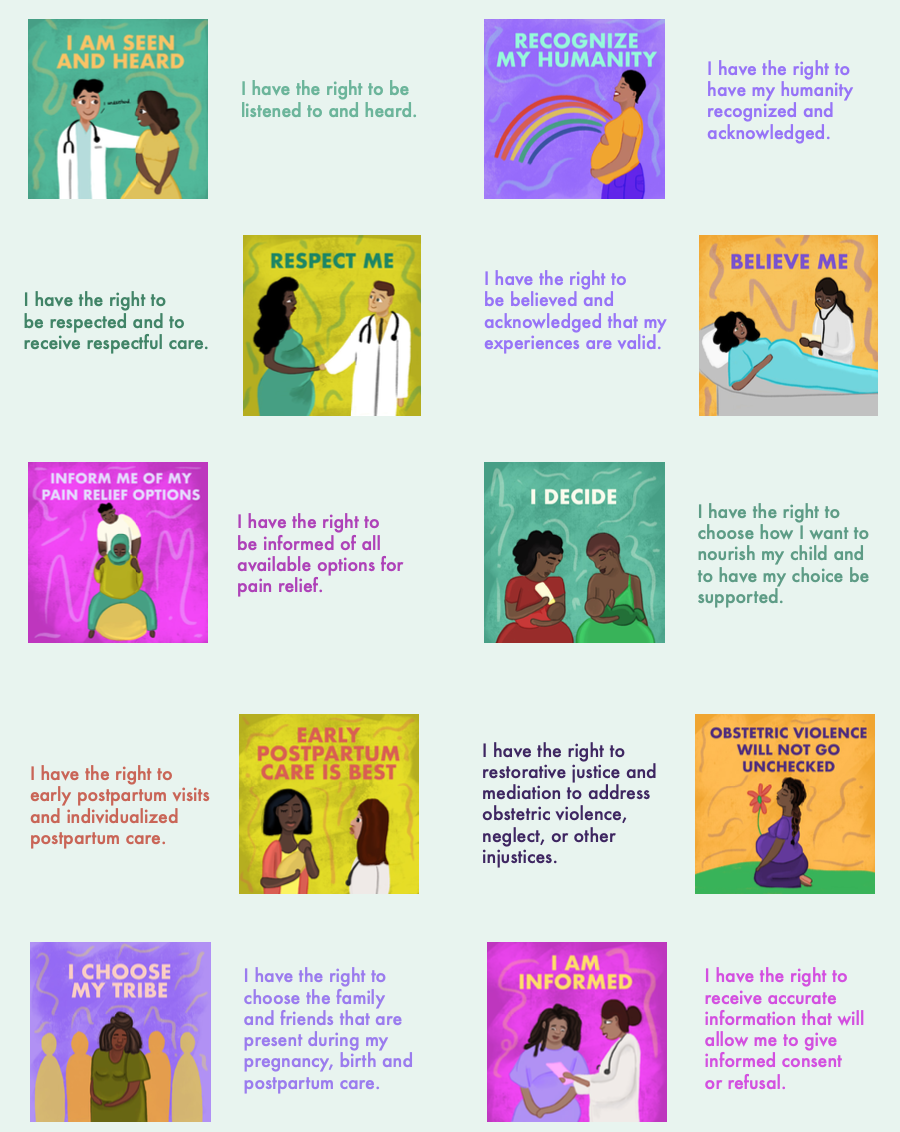
What matters to birthing patients is:
- Giving birth to a healthy baby in a clinically and psychologically safe environment
- Practical and emotional support from birth companions and competent, reassuring, kind clinical staff
- Individualized care
- Sense of personal achievement and control through active decision-making
Birth Setting
Possible birth settings include hospital, home, or birth center birth. There are advantages and disadvantages to all three settings, and may patients' options are limited/controlled by financial and insurance decisions rather than personal decision-making. Whereas the hospital setting has demonstrated benefit in "high risk" deliveries, there is plenty of data showing that both home birth and birth center birth can be just as safe in "low risk" patients. Whereas hospitals offer expert and facile access to testing and timely interventions, they tend to be less private, less comfortable and allow limited freedom of movement. Birth centers have demonstrated less interventions and some improved outcomes with similar safety outcomes to hospital birth in a select patient population.



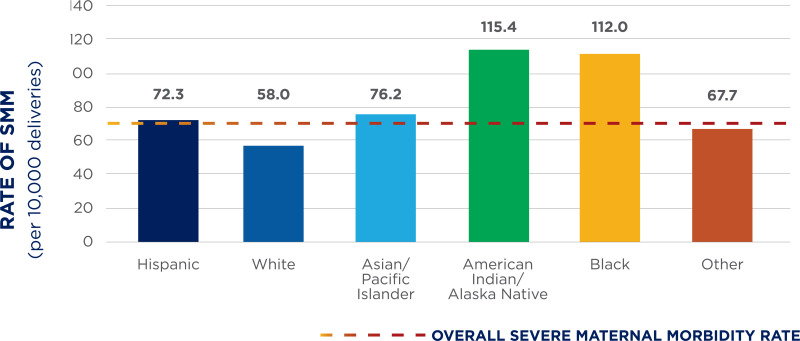
Racial and ethnic disparities exist. As we know, BIPOC women have increased rates of maternal mortality but also have increased rates of discrimination and mistreatment in the hospital setting, including higher rates of feeling "pressured into interventions". In one study, 30% of BIPOC patients experience mistreatment during hospital birth compared to 6.6% of patients who delivered in a birth center.
***
There are many evidence-based and non-evidence based interventions patients and providers use/recommend to promote physiologic birth. These very across the stages of labor. Dr. Saedi-Kwon reviewed briefly the use and evidence for these interventions/options:
First stage of labor
"natural birth preparation" or "natural induction"
- Red raspberry tea
- Dates
- Castor oil
- Primrose oil

Pain Management is an important consideration for laboring patients. IVs, medications, and pharmaceutical interventions can have a tethering effect for women, and non-pharmacological interventions have some high level evidence. These include:
- Continuous labor support (i.e. doulas and/or partner support): associated with decreased length of labor, increased rates of vaginal birth, reduced procedural deliveries, decreased pain medications and increased patient satisfaction. Continuous labor support also allows someone to be present who is advocating for the patient during their labor. Of note, Medi-Cal now covers doula services.
- maternal position: upright and walking has demonstrated better outcomes
- hydrotherapy/water immersion: decreases anxiety and improves pain without any evidence of harm
- counter pressure: mixed data but some studies show improved pain scores
How can we limit interventions in birth?
- Delayed admission to L&D
- Outpatient cervical ripening: pharm or non-pharm placed in the hospital (misoprostol or foley) with return in 12-24 hour for recheck
- Whereas current guidelines do recommend immediate induction of labor if a patient has PROM, 95% of patients with PROM will go into spontaneous labor within 24-48 hours
- Intermittent auscultation for fetal monitoring (via doppler)
2nd Stage of Labor
- Perineal massage: metanalysis found a decrease rates of 3rd and 4th degree lacerations, more significant in primigravida
- starting at 34 weeks, 3-9 o'clock posterior perineum, clean hands, lubricant (water-based or food based oil)
- can by done by partner or self
- even as infrequently as 1-2x week has benefit
- Warm compresses held to perineum during/between pushing also has some evidence of decreased 3rd/4th degree lacerations
- "Hands on" vs. "Hands poised" position (by provider): mixed evidence, comparing the two, hands on shows no reduction in anal sphincter injury
- Pushing (studies done in patients with epidurals)
- immediate vs. delayed, immediate pushing does decrease length of second stage and reduces rates of chorioamnionitis, but there is no different in vaginal operative delivery, laceration, or post-partum hemorrhage
- open vs. closed glottis: closed glottis does again decrease length of second stage but does also increase risk of abnormal post partum urodynamics
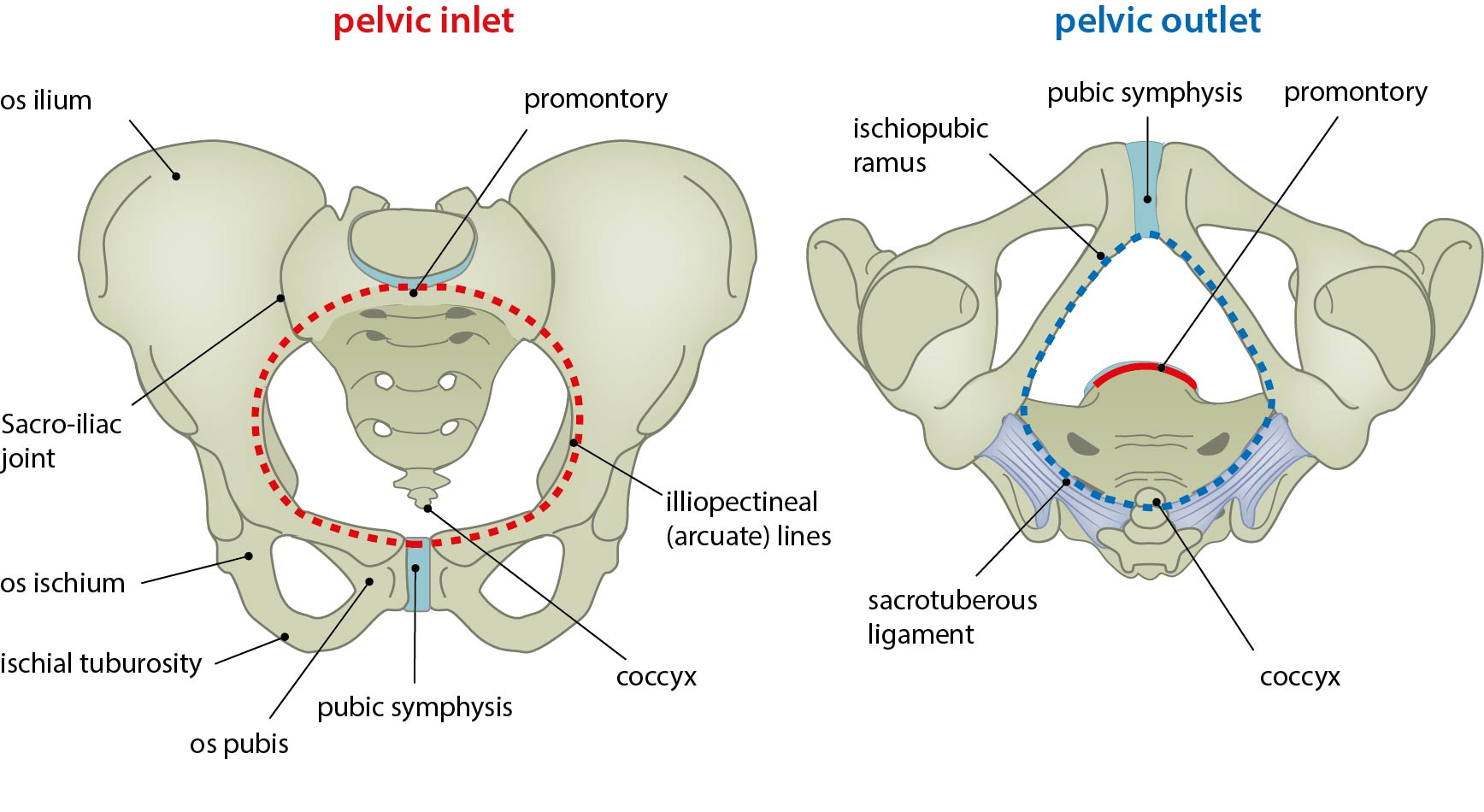
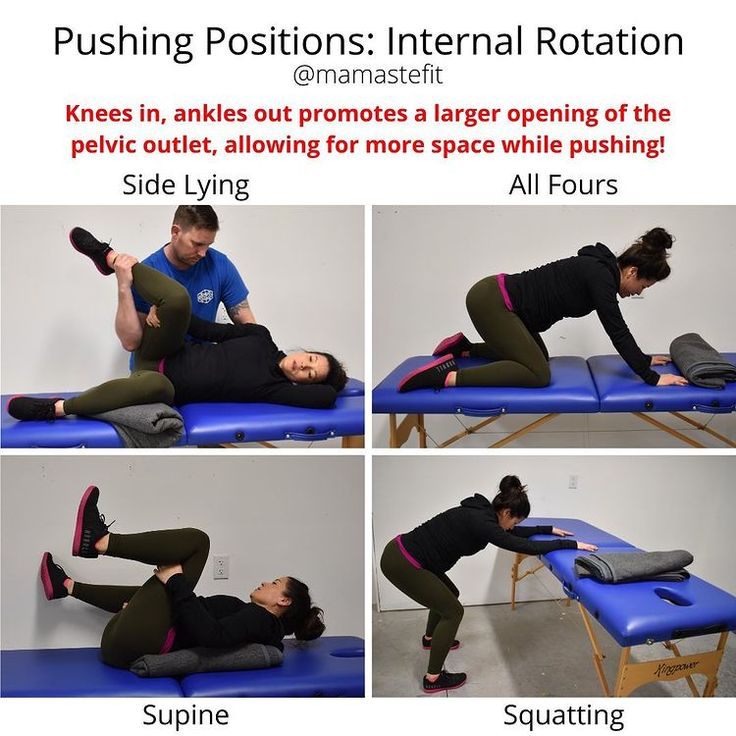
- opening the pelvis with knees wide (traditional lithotomy) vs. with internal rotation of the knees: internal rotation does increase size of pelvic outlet
- pushing position: upright and side lying (as opposed to lithotomy) does increase rates of intact perineum
3rd Stage of Labor
- Delayed cord clamping increased final blood volume of neonate by 20-30% and has proven benefit in neonates, >120 seconds
- in very preterm neonates (<28 weeks), cord milking may be preferred to allow for urgent resuscitation for non-vigorous infants
- To decrease rates of postpartum hemorrhage (PPH):
- Pitocin at delivery of anterior shoulder decreases rates of severe PPH
- cord traction with counterpressure on uterus (risks are cord avulsion (5%)and uterine inversion (<0.1%), both of which are rare



No comments:
Post a Comment