A recording of this week's Grand Rounds is available HERE.
This was an excellent presentation by a pediatric allergist, Dr. John Kelso. I learned a lot, but I'm a little behind on writing up a summary.
Check back for my notes shortly.

A recording of this week's Grand Rounds is available HERE.
This was an excellent presentation by a pediatric allergist, Dr. John Kelso. I learned a lot, but I'm a little behind on writing up a summary.
Check back for my notes shortly.
A recording of this presentation is available HERE.
Thanks to Dr. Ryley Saedi-Kwon for her presentation this week on Physiologic Birth. As usual, a recording of the presentation is available above. Dr. Saedi-Kwon covered a wide range of birth topics, see my highlights below.
Physiologic Birth, as outlined in a 2012 consensus statement of US midwifery organizations includes:
2018 systematic qualitative review found that
Most wanted a physiological labor and birth while acknowledging that birth can be unpredictable and frightening and they may need to ‘go with the flow’
Small minority birth was physical process that should be conducted as quickly and painlessly as possible




A recording of this presentation is available HERE.
Many thanks to Dr. Connie Earl for a FANTASTIC Grand Rounds presentation this week on Osteopathic Manipulation in the Hospital. Dr. Earl, who previously ran the Forestville Wellness Center through West County Health Centers, is currently doing a year of extra "residency" training on Osteopathic and Neuromuscular Medicine (ONMN) at Maine Medical Center. She shared with us her passion for Osteopathic Manipulation (OMM/OMT) and a TON of what she described as "really weird studies that demonstrate ways in which OMN may be used in the hospital setting".
As an allopathic-trained physician, I admit I am often envious of the anatomy knowledge and tremendous skills of my osteopathic colleagues-- and I can tell you from personal experience that Dr. Earl has amazing clinical skills (and hands!)
For those of us less familiar with OMT, she started with the four principles of osteopathy:
The body is a unit; the person is a unit of body, mind and spirit.
The body is capable of self-regulation, self-healing and health maintenance.
Structure and function are reciprocally interrelated.
Rational treatment is based upon an understanding of the basic principles of body unity, self-regulation and the interrelationship of structure and function.



A recording of this presentation is available HERE.

My notes:
Hemorrhoids are extremely common -- 5-10% of the population, >2.2 million people per year with over 2 million prescriptions per year that add up to over $43 million in healthcare costs. But many patients are being treated for hemorrhoids when there may be other things going on down there, including: fissures, fistula, abscess, pruritis, and rectal prolapse.
Dr. Cortez reminded us to go back to the basics: 1) listen to the patient (e.g. hemorrhoids generally don't hurt, so if the patient is complaining of pain, broaden your ddx) and 2) examine the patient.
Fiber
Encourage fiber! All our patients need more fiber. And fiber isn't good for just the perianal region. Fiber decreases risk of cardiovascular disease, decreases risk for colon cancer. "The best fiber out there is the one you'll take". Really, the only downside is increased flatulence.
Fiber options abound, including: psyllium husk, benefiber (can sprinkle on yogurt), fiber capsules or gummies (e.g. Kirkland brand, 2-4 gummies 2x per day, with LOTS of water).
Once you start a fiber supplement, don't make any changes for 5 days.
Miralax is good too, but it shouldn't replace fiber. Use miralax PRN for constipation.
Dr. Cortez reminded us that the increased pressure of diarrhea can also contribute to hemorrhoids. The goal is ONE nice big healthy bowel movement per day, no more than 4-5 minutes sitting on the pot. It is better to return 3 or more times than sit for prolonged period of time on the toilet.
When you are going to examine a patient for perianal complaints: put them in L lateral decubitus (better to see than lithotomy). Look externally for tags, fissures/openings, thickened skin, ulcerations, masses. If you see a fissure stop there (you can make it worse). Use anoscopy and a digital exam to check for tone, masses, blood, etc.
Dr. Cortez is not a fan of donuts for any perianal condition. In his eloquent words: "Gravity tries to push your liver right out your butt"
Hemorrhoid Treatment
1) Banding (in office), no prep, effective, can be done several times, no downtime, no severe pain
2) Hemorrhoidectomy (surgical) is always a last resort, very pain ful but most effective. Stapled hemorrhoidectomies are not superior.
Thrombosed hemorrhoids, which present as big purple extremely painful lumps should be unroofed in first 2-3 days for pain control (in ED or office). If it has been > 5 days, healing is equivalent and intervention is not indicated.
Fissures
Perianal fissures, which are tears in the anoderm exposing the sphincter muscles, are extremely painful. Patients may describe symptoms as "crapping out glass" or "jamming a knife in my butt". 73% present midline posteriorly. If you visualize a lateral fissure, that patient needs a work-up, including testing for Crohn's, HIV, syphillis, TB and more.

Acute fissures (< 6 months) can be treated with fiber, fiber and fiber, as well as hydration and sitz baths. This takes time! Topicals can sooth and manage symptoms, including topical nitroglycerine. Dr. Cortez's preferred topical is compounded diltiazem/nifedipine cream (locally can get compounded at Dollar Drug). Can be rx'd TID.
Chronic fissures (>6 months) require treatment with chemo-denervation, including Botox, which is effective and stops spasm. Some people need surgical intervention: with sphincterotomy or anocutaneous flap.
Perianal abscess
Perianal abscesses can also be extremely painful. 30-70% of abscesses have an accompanying fistula. 40-50% will develop a fistula over time.

Malignancy
Finally, malignancies can present in the perianal region and the only way to diagnose them is to look for them. These can include squamous cell carcinomas and melanomas. See images below for some examples.

A recording of this presentation is available HERE.
***
This was a mind-blowing and practice-changing Grand Rounds this week -- so much to learn and understand about vaping (aka e-cigarettes) as primary care providers. The speaker, Dr. Pamela Ling, is the Director of the UCSF Center for Tobacco Research and Education, and she shared so much valuable data and on-the-ground information about the current state of vaping. The title of her talk was Vaping: Medicine or Menace?
Here's what I learned:
First off, the vaping industry is rapidly evolving. Unfortunately, the science, while forthcoming, lags behind an agile and sneaky industry. The first e-cigarettes came on the market in 2009 and looked like little "fake cigarettes" (they even featured a puff of smoke). Now, vapes come in a shapes and sizes and with increasingly concentrated (and flavored) solutions and changing delivery devices.

E-cigarettes create an aerosol by using a battery to heat up liquid that usually contains nicotine, flavoring, and other additives. Users inhale this aerosol into their lungs. E-cigs can also be used to deliver cannabinoids, such as marijuana and other drugs.
OMG check this out! These are vaping products confiscated from high schools in California and North Carolina (1000 products from 25 high schools) from an MMWR publication.
 |





In addition to vaping nicotine, cannabis is increasingly popular; almost as many people use cannabis as tobacco now in the US. And while smoking is still the most common way to consume cannabis, edibles and vaping are both increasing.


It is important to understand that there is SOME evidence of the use of e-cigarettes to promote smoking cessation, though the evidence is weak at best. E cigarettes are not approved by the FDA for smoking cessation, though they are recommended by the UK NHS due to this evidence. Under RCT conditions, earlier generations of vape products have been shown to be more effective than nicotine replacement therapy. You can see this data below summarized in the Cochrane review below.

This has not borne out in population level observational studies-- in other words, when used as a consumer product, e-cigarettes do not help with cessation. Also important to note that the e-cig market is evolving extremely rapidly and the products are increasingly appealing to young people (this is not a coincidence).

Isn't vaping better for us than smoking?
Stella Tomassi and colleagues published a study of young adult vapers who never smoked compared to smokers using quantitative PCR to detect DNA damage (as a marker for future cancer). They found a dose-dependent formation of DNA damage in oral cells of vapers who had never smoked tobacco cigarettes as well as exclusive cigarette smokers. They also found more damage seen in heavier users, users of pod vapes and sweet flavors) independent of nicotine levels.
Recent studies of the epigenetic effects of tobacco smoking and e-cigarette use found similar changes in DNA methylation among people using cigarettes and people using e-cigarettes, changes that were associated with lung carcinogenesis.
While we do not have direct human data on vaping and lung cancer outcomes, these newer biomarkers of DNA damage and epigenetic changes are likely to be informative for lung cancer risk.
In terms of cardiovascular disease: a recent study published in NEJM 2024 found that CV disease risk from vaping was NO different than CV disease risk from smoking. So for CV risk the answer is NO.
But here's perhaps one of the most important take home points: dual use (using BOTH vapes and cigarettes) is definitely the worst for patients. Check out this summary table below showing the risk of disease appears higher for dual users. . .

A recording of this presentation is available HERE.
Deep gratitude for our two Addiction Medicine Fellows, Drs. Bianka Aguilar and Anna Bowen, for an important and concrete presentation this week on Methadone in Hospitalized patients. They will be back in the spring with another Addiction Medicine presentation!
Here are my favorite pearls:
1) Starting methadone in the hospital decreases self-directed (AMA) discharges (30% vs. 59.6%), reduces all-cause readmission rates (27% vs. 41%), and decreases risk of endocarditis, osteomyelitis, and septic arthritis. I was taught that we should be "cautious" in the hospital about starting methadone if there wasn't a long-term plan for follow-up, but this is no longer true. If a patient is motivated to start methadone and it is indicated, we should do it. There are many new algorithms that can cross taper people easily from methadone to buprenorphine IF they are unable to get methadone through an outpatient treatment center.
2) Fentanyl in our drug supply has changed the treatment of opioid use disorder (OUD). Recent studies are showing the methadone may be superior to buprenorphine in terms of treating OUD in fentanyl users. Methadone for OUD also appears to have higher retention rates.

4) While methadone is known to lengthen the QT interval, not everyone on methadone needs serial or even baseline EKG monitoring. Most guidelines recommend an EKG at initiation of methadone only for patients with other cardiac risk factors (e.g. known prolonged QT, CAD, CHF, etc.) AND once methadone doses near 100mg daily. This is a dose response side effect. We should remember to look at other medications that can also prolong QTc to see if those can be altered/discontinued. A QTc of >500 is not an absolute contraindication to treating with methadone, but the clinical scenario merits review (e.g. medication review)
4) Some people are "rapid metabolizers", meaning that single daily dose of methadone may be insufficient to help with cravings and treat their opiate use disorder. This is known to be true in pregnancy, but can also occur in some patients. Rapid metabolizing most often manifest as someone who appears appropriately treated by a certain methadone dose by 2-4 hours after their dose (maybe even a little sedated), but then 12 hours later is experiencing s/sx of withdrawal or cravings. We can potentially help their case to receive methadone BID by checking "peak" (2-4 hours after the dose) and "trough" (right BEFORE their dose) serum level of methadone.

Practical tips for methadone in hospitalized patients:

 |
| Toronto Perinatal Addiction Medicine Team |
A recording of this presentation is available HERE.
Many thanks to Dr. Andrew Brown, who gave an excellent Grand Rounds presentation this week on Integrative Approach to Anxiety and Depression. Anyone in primary care knows that we do a lot of management of psychiatric disorders in the primary care setting, often with very little specialty support. Many patients are interested in pursuing not just standard medical therapy (SSRI + cognitive behavioral therapy), but also integrative modalities.
Dr. Brown laid out the evidence for a wide range of non-pharmaceutical and non-psychotherapy treatments for anxiety and depression. The bottom line is that there are many, many, many integrative options with a range of small to moderate to strong evidence for the management of anxiety/depression. Put your seatbelts on. And don't use too many at once!
Integrative modalities, for the purpose of this talk include
Lifestyle/behavioral
Exercise works! The USPSTF recommends 2.5 hours/week of aerobic exercise for overall improved health. And good news, exercise can improved depression! Some exercise modalities may be better than others, including: include walking/jogging/yoga/strength training. The more "intense" the better. However, in a 2023 review article, ANY regular exercise, regardless of type, setting, or supervision decreased depression scores by 5-7 points.
There is not much evidence for exercise in anxiety, with a different review paper finding a benefit of exercise for anxiety in 7 of 25 studies and no benefit in the remaining 18.
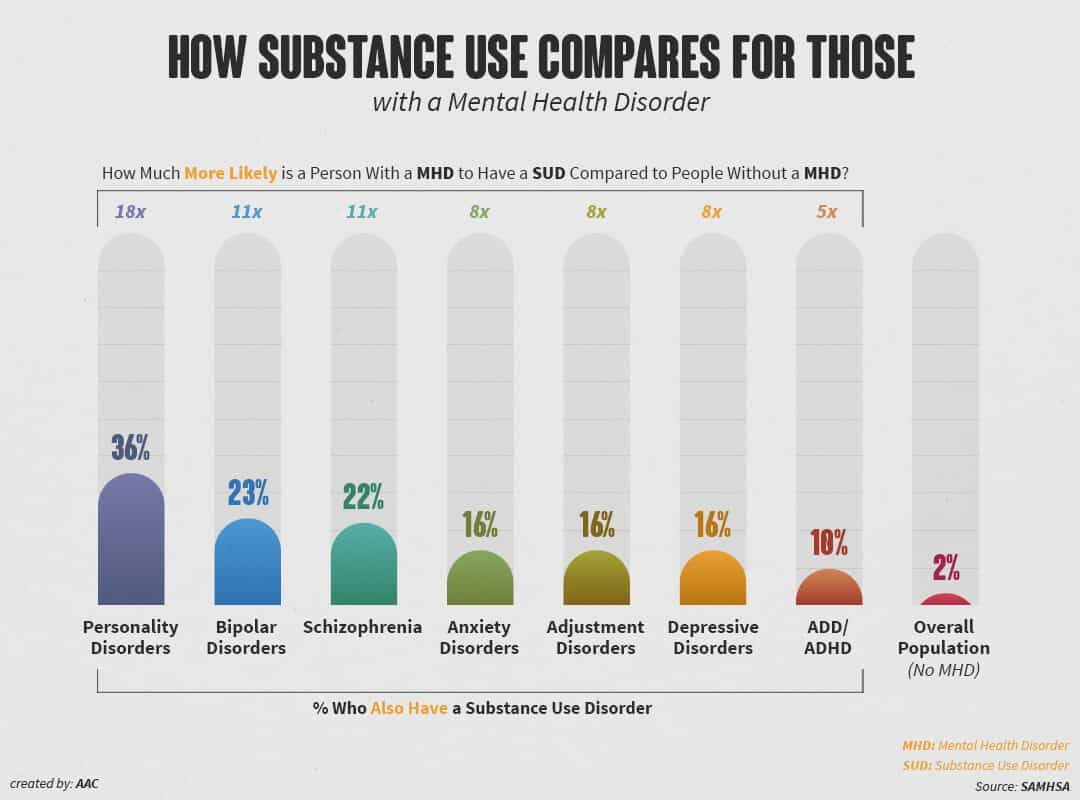
It should come as no surprise that substance use and substance use disorders are frequent comorbidities with anxiety and depression. Note in the chart below:





de Noronha, S.I.S.R., de Moraes, L.A.G., Hassell, J.E. et al. High-fat diet, microbiome-gut-brain axis signaling, and anxiety-like behavior in male rats. Biol Res 57, 23 (2024). https://doi.org/10.1186/s40659-024-00505-1
Fatemi, F., Siassi, F., Qorbani, M. et al. Higher dietary fat quality is associated with lower anxiety score in women: a cross-sectional study. Ann Gen Psychiatry 19, 14 (2020). https://doi.org/10.1186/s12991-020-00264-9
Mohit Kumar, Babita Bhatt, Chitralekha Gusain, Nayan Mahajan, Mahendra Bishnoi, Sex-specific effects of ketogenic diet on anxiety-like behavior and neuroimmune response in C57Bl/6J mice, The Journal of Nutritional Biochemistry, Volume 127 (2024). https://doi.org/10.1016/j.jnutbio.2024.109591.
Haduch, A.; Bromek, E.; Kuban, W.; Daniel, W.A. The Engagement of Cytochrome P450 Enzymes in Tryptophan Metabolism. Metabolites 2023, 13, 629. https://doi.org/10.3390/metabo13050629
Gregory L. Stonerock, Rahul P. Gupta, James A. Blumenthal, Is exercise a viable therapy for anxiety? Systematic review of recent literature and critical analysis, Progress in Cardiovascular Diseases, Volume 83, 2024, Pages 97-115, https://doi.org/10.1016/j.pcad.2023.05.006.
Noetel M, Sanders T, Gallardo-Gómez D, Taylor P, del Pozo Cruz B, van den Hoek D et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials BMJ 2024; 384 :e075847 https://doi:10.1136/bmj-2023-075847
Kedzior, K.K., Laeber, L.T. A positive association between anxiety disorders and cannabis use or cannabis use disorders in the general population- a meta-analysis of 31 studies. BMC Psychiatry 14, 136 (2014). https://doi.org/10.1186/1471-244X-14-136
Berglund, M. and Ojehagen, A. (1998), The Influence of Alcohol Drinking and Alcohol Use Disorders on Psychiatric Disorders and Suicidal Behavior. Alcoholism: Clinical and Experimental Research, 22: 333s-345s. https://doi.org/10.1111/j.1530-0277.1998.tb04388.x
Lev-Ran S, Roerecke M, Le Foll B, George TP, McKenzie K, Rehm J. The association between cannabis use and depression: a systematic review and meta-analysis of longitudinal studies. Psychological Medicine. 2014;44(4):797-810. doi:10.1017/S0033291713001438
Pinto JV, Crippa JAS, Ceresér KM, Vianna-Sulzbach MF, Silveira Júnior ÉM, Santana da Rosa G, Testa da Silva MG, Hizo GH, Simão Medeiros L, Santana de Oliveira CE, Bristot G, Campos
AC, Guimarães FS, Hallak JEC, Zuardi AW, Yatham LN, Kapczinski F, Kauer-Sant'Anna M. Cannabidiol as an Adjunctive Treatment for Acute Bipolar Depression: A Pilot Study: Le cannabidiol comme traitement d'appoint de la dépression bipolaire aiguë : une étude pilote. Can J Psychiatry. 2024 Apr;69(4):242-251. doi: 10.1177/07067437231209650. Epub 2023 Nov 3. PMID: 37920963; PMCID: PMC10924581.
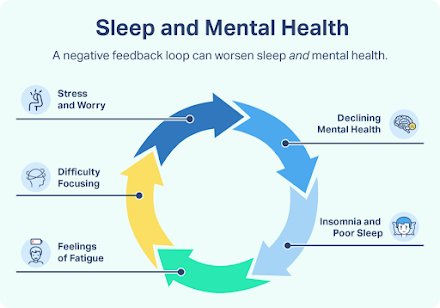
Gebara MA, Siripong N, DiNapoli EA, Maree RD, Germain A, Reynolds CF, Kasckow JW, Weiss PM, Karp JF. Effect of insomnia treatments on depression: A systematic review and meta-analysis. Depress Anxiety. 2018 Aug;35(8):717-731. doi: 10.1002/da.22776. Epub 2018 May 21. PMID: 29782076.
Fava M, Schaefer K, Huang H, Wilson A, Iosifescu DV, Mischoulon D, Wessel TC. A post hoc analysis of the effect of nightly administration of eszopiclone and a selective serotonin reuptake inhibitor in patients with insomnia and anxious depression. J Clin Psychiatry. 2011 Apr;72(4):473-9. doi: 10.4088/JCP.09m05131gry. Epub 2010 Nov 2. PMID: 21208574.
Nagy E, Moore S. Social interventions: An effective approach to reduce adult depression? J Affect Disord. 2017 Aug 15;218:131-152. doi: 10.1016/j.jad.2017.04.043. Epub 2017 Apr 24. PMID: 28472703.
Cruwys T, Alexander Haslam S, Dingle GA, Jetten J, Hornsey MJ, Desdemona Chong EM, Oei TP. Feeling connected again: interventions that increase social identification reduce depression symptoms in community and clinical settings. J Affect Disord. 2014 Apr;159:139-46. doi: 10.1016/j.jad.2014.02.019. Epub 2014 Feb 18. PMID: 24679402.
Beauchamp AM, Lehmann CU, Medford RJ, Hughes AE. The Association of a Geographically Wide Social Media Network on Depression: County-Level Ecological Analysis. J Med Internet Res. 2023 Mar 27;25:e43623. doi: 10.2196/43623. Erratum in: J Med Internet Res. 2023 Apr 11;25:e47896. doi: 10.2196/47896. PMID: 36972109; PMCID: PMC10131939.
Primack BA, Bisbey MA, Shensa A, Bowman ND, Karim SA, Knight JM, Sidani JE. The association between valence of social media experiences and depressive symptoms. Depress Anxiety. 2018 Aug;35(8):784-794. doi: 10.1002/da.22779. Epub 2018 Jun 6. PMID: 29877002.
Mizumoto T, Ikei H, Hagiwara K, Matsubara T, Higuchi F, Kobayashi M, Yamashina T, Sasaki J, Yamada N, Higuchi N, Haraga K, Kirihara F, Okabe E, Asai K, Hirotsu M, Chen C, Miyazaki Y, Nakagawa S. Mood and physiological effects of visual stimulation with images of the natural environment in individuals with depressive and anxiety disorders. J Affect Disord. 2024 Jul 1;356:257-266. doi: 10.1016/j.jad.2024.04.025. Epub 2024 Apr 7. PMID: 38588725.
Yeon PS, Jeon JY, Jung MS, Min GM, Kim GY, Han KM, Shin MJ, Jo SH, Kim JG, Shin WS. Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2021 Dec 1;18(23):12685. doi: 10.3390/ijerph182312685. PMID: 34886407; PMCID: PMC8657257.
https://medicine.umich.edu/sites/default/files/content/downloads/Relaxation-Skills-for-Anxiety.pdf
Heissel A, Heinen D, Brokmeier LL, Skarabis N, Kangas M, Vancampfort D, Stubbs B, Firth J, Ward PB, Rosenbaum S, Hallgren M, Schuch F. Exercise as medicine for depressive symptoms? A systematic review and meta-analysis with meta-regression. Br J Sports Med. 2023 Aug;57(16):1049-1057. doi: 10.1136/bjsports-2022-106282. Epub 2023 Feb 1. PMID: 36731907; PMCID: PMC10423472.
Gartlehner G, Dobrescu A, Chapman A, Toromanova A, Emprechtinger R, Persad E, Affengruber L, Pieh C, Klerings I, Wagner G. Nonpharmacologic and Pharmacologic Treatments of Adult Patients With Major Depressive Disorder: A Systematic Review and Network Meta-analysis for a Clinical Guideline by the American College of Physicians. Ann Intern Med. 2023 Feb;176(2):196-211. doi: 10.7326/M22-1845. Epub 2023 Jan 24. PMID: 36689750.
Sarris J, Marx W, Ashton MM, Ng CH, Galvao-Coelho N, Ayati Z, Zhang ZJ, Kasper S, Ravindran A, Harvey BH, Lopresti A, Mischoulon D, Amsterdam J, Yatham LN, Berk M. Plant-based Medicines (Phytoceuticals) in the Treatment of Psychiatric Disorders: A Meta-review of Meta-analyses of Randomized Controlled Trials: Les médicaments à base de plantes (phytoceutiques) dans le traitement des troubles psychiatriques: une méta-revue des méta-analyses d'essais randomisés contrôlés. Can J Psychiatry. 2021 Oct;66(10):849-862. doi: 10.1177/0706743720979917. Epub 2021 Feb 18. PMID: 33596697; PMCID: PMC8573706.
Jacobs B.P., Bent S., Tice J.A., Blackwell T., Cummings S.R. An internet-based randomized, placebo-controlled trial of kava and valerian for anxiety and insomnia. Medicine. 2005;84:197–207. doi: 10.1097/01.md.0000172299.72364.95.
Hausenblas H.A., Saha D., Dubyak P.J., Anton S.D. Saffron (Crocus sativus L.) and major depressive disorder: A meta-analysis of randomized clinical trials. J. Integr. Med. 2013;11:377–383. doi: 10.3736/jintegrmed2013056.
Lopresti A.L., Drummond P.D. Saffron (Crocus sativus) for depression: A systematic review of clinical trials and examination of underlying antidepressant mechanisms of action. Hum. Psychopharmacol. 2014;29:517–527. doi: 10.1002/hup.2434.
Kasper S., Gastpar M., Müller W.E., Volz H.P., Möller H.J., Schläfke S., Dienel A. Lavender oil preparation Silexan is effective in generalized anxiety disorder-A randomized, double-blind comparison to placebo and paroxetine. Int. J. Neuropsychopharmacol. 2014;17:859–869. doi: 10.1017/S1461145714000017.
Kasper S., Anghelescu I., Dienel A. Efficacy of orally administered Silexan in patients with anxiety-related restlessness and disturbed sleep—A randomized, placebo-controlled trial. Eur. Neuropsychopharmacol. 2015;25:1960–1967. doi: 10.1016/j.euroneuro.2015.07.024.
Kasper S., Volz H.P., Dienel A., Schläfke S. Efficacy of Silexan in mixed anxiety-depression-A randomized, placebo-controlled trial. Eur. Neuropsychopharmacol. 2016;26:331–340. doi: 10.1016/j.euroneuro.2015.12.002
Woelk H., Schläfke S. A multi-center, double-blind, randomised study of the Lavender oil preparation Silexan in comparison to Lorazepam for generalized anxiety disorder. Phytomedicine. 2010;17:94–99. doi: 10.1016/j.phymed.2009.10.006.
Janda K., Wojtkowska K., Jakubczyk K., Antoniewicz J., Skonieczna-żydecka K. Passiflora incarnata in Neuropsychiatric Disorders—A Systematic Review. Nutrients. 2020;12:3894. doi: 10.3390/nu12123894.
Sarris J, Kavanagh DJ, Byrne G, Bone KM, Adams J, Deed G. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of Piper methysticum. Psychopharmacology (Berl). 2009 Aug;205(3):399-407. doi: 10.1007/s00213-009-1549-9. Epub 2009 May 9. PMID: 19430766.
Liu RT, Walsh RFL, Sheehan AE. Prebiotics and probiotics for depression and anxiety: A systematic review and meta-analysis of controlled clinical trials. Neurosci Biobehav Rev. 2019 Jul;102:13-23. doi: 10.1016/j.neubiorev.2019.03.023. Epub 2019 Apr 17. PMID: 31004628; PMCID: PMC6584030.
Yang Y, Yang L, Wan M, Pan D, Sun G, Yang C. Assessment of optimal combinations of therapeutic probiotics for depression, anxiety, and stress. Psychol Med. 2024 Jul;54(10):2547-2561. doi: 10.1017/S0033291724000679. Epub 2024 Mar 18. PMID: 38497101.
Yosaee S, Clark CCT, Keshtkaran Z, Ashourpour M, Keshani P, Soltani S. Zinc in depression: From development to treatment: A comparative/ dose response meta-analysis of observational studies and randomized controlled trials. Gen Hosp Psychiatry. 2022 Jan-Feb;74:110-117. doi: 10.1016/j.genhosppsych.2020.08.001. Epub 2020 Aug 10. PMID: 32829928.
Ranjbar E, Kasaei MS, Mohammad-Shirazi M, Nasrollahzadeh J, Rashidkhani B, Shams J, Mostafavi SA, Mohammadi MR. Effects of zinc supplementation in patients with major depression: a randomized clinical trial. Iran J Psychiatry. 2013 Jun;8(2):73-9. PMID: 24130605; PMCID: PMC3796297.
Tarleton EK, Littenberg B, MacLean CD, Kennedy AG, Daley C. Role of magnesium supplementation in the treatment of depression: A randomized clinical trial. PLoS One. 2017 Jun 27;12(6):e0180067. doi: 10.1371/journal.pone.0180067. PMID: 28654669; PMCID: PMC5487054.
Wang H, Jin M, Xie M, Yang Y, Xue F, Li W, Zhang M, Li Z, Li X, Jia N, Liu Y, Cui X, Hu G, Dong L, Wang G, Yu Q. Protective role of antioxidant supplementation for depression and anxiety: A meta-analysis of randomized clinical trials. J Affect Disord. 2023 Feb 15;323:264-279. doi: 10.1016/j.jad.2022.11.072. Epub 2022 Nov 25. PMID: 36442656.
Borges-Vieira JG, Cardoso CKS. Efficacy of B-vitamins and vitamin D therapy in improving depressive and anxiety disorders: a systematic review of randomized controlled trials. Nutr Neurosci. 2023 Mar;26(3):187-207. doi: 10.1080/1028415X.2022.2031494. Epub 2022 Feb 14. PMID: 35156551.
Zhu C, Zhang Y, Wang T, Lin Y, Yu J, Xia Q, Zhu P, Zhu DM. Vitamin D supplementation improves anxiety but not depression symptoms in patients with vitamin D deficiency. Brain Behav. 2020 Nov;10(11):e01760. doi: 10.1002/brb3.1760. Epub 2020 Sep 18. PMID: 32945627; PMCID: PMC7667301.
Wang R, Xu F, Xia X, Xiong A, Dai D, Ling Y, Sun R, Qiu L, Ding Y, Xie Z. The effect of vitamin D supplementation on primary depression: A meta-analysis. J Affect Disord. 2024 Jan 1;344:653-661. doi: 10.1016/j.jad.2023.10.021. Epub 2023 Oct 16. PMID: 37852593.
Marschall J, Fejer G, Lempe P, Prochazkova L, Kuchar M, Hajkova K, van Elk M. Psilocybin microdosing does not affect emotion-related symptoms and processing: A preregistered field and lab-based study. J Psychopharmacol. 2022 Jan;36(1):97-113. doi: 10.1177/02698811211050556. Epub 2021 Dec 17. PMID: 34915762; PMCID: PMC8801668.
Tan Y, Duan R, Wen C. Efficacy of acupuncture for depression: a systematic review and meta-analysis. Front Neurosci. 2024 Apr 30;18:1347651. doi: 10.3389/fnins.2024.1347651. PMID: 38745939; PMCID: PMC11091333.
Zhichao H, Ching LW, Huijuan L, Liang Y, Zhiyu W, Weiyang H, Zhaoxiang B, Linda ZLD. A network meta-analysis on the effectiveness and safety of acupuncture in treating patients with major depressive disorder. Sci Rep. 2021 May 17;11(1):10384. doi: 10.1038/s41598-021-88263-y. PMID: 34001924; PMCID: PMC8129113.
Xu G, Lei H, Huang L, Xiao Q, Huang B, Zhou Z, Tian H, Huang F, Liu Y, Zhao L, Li X, Liang F. The dose-effect association between acupuncture sessions and its effects on major depressive disorder: A meta-regression of randomized controlled trials. J Affect Disord. 2022 Aug 1;310:318-327. doi: 10.1016/j.jad.2022.04.155. Epub 2022 May 2. PMID: 35504399.
Xu Z, Zhang X, Shi H, Liang M, Ning F, Wang Q, Jia H. Efficacy of acupuncture for anxiety and depression in functional dyspepsia: A systematic review and meta-analysis. PLoS One. 2024 Mar 7;19(3):e0298438. doi: 10.1371/journal.pone.0298438. PMID: 38452033; PMCID: PMC10919749.
Carlson LE, Ismaila N, Addington EL, Asher GN, Atreya C, Balneaves LG, Bradt J, Fuller-Shavel N, Goodman J, Hoffman CJ, Huston A, Mehta A, Paller CJ, Richardson K, Seely D, Siwik CJ, Temel JS, Rowland JH. Integrative Oncology Care of Symptoms of Anxiety and Depression in Adults With Cancer: Society for Integrative Oncology-ASCO Guideline. J Clin Oncol. 2023 Oct 1;41(28):4562-4591. doi: 10.1200/JCO.23.00857. Epub 2023 Aug 15. PMID: 37582238.
Fan JQ, Lu WJ, Tan WQ, Liu X, Wang YT, Wang NB, Zhuang LX. Effectiveness of Acupuncture for Anxiety Among Patients With Parkinson Disease: A Randomized Clinical Trial. JAMA Netw Open. 2022 Sep 1;5(9):e2232133. doi: 10.1001/jamanetworkopen.2022.32133. PMID: 36129711; PMCID: PMC9494193.
Wiles MD, Mamdani J, Pullman M, Andrzejowski JC. A randomised controlled trial examining the effect of acupuncture at the EX-HN3 (Yintang) point on pre-operative anxiety levels in neurosurgical patients. Anaesthesia. 2017 Mar;72(3):335-342. doi: 10.1111/anae.13785. Epub 2017 Jan 16. PMID: 28092106.
Molassiotis A, Suen L, Lai C, Chan B, Wat KHY, Tang J, To KL, Leung CO, Lee S, Lee P, Chien WT. The effectiveness of acupressure in the management of depressive symptoms and in improving quality of life in older people living in the community: a randomised sham-controlled trial. Aging Ment Health. 2020 Jun;24(6):1001-1009. doi: 10.1080/13607863.2019.1584789. Epub 2019 Mar 14. PMID: 30869991.
Linardon J, Messer M, Goldberg SB, Fuller-Tyszkiewicz M. The efficacy of mindfulness apps on symptoms of depression and anxiety: An updated meta-analysis of randomized controlled trials. Clin Psychol Rev. 2024 Feb;107:102370. doi: 10.1016/j.cpr.2023.102370. Epub 2023 Dec 3. PMID: 38056219; PMCID: PMC10872959.
Hofmann SG, Gómez AF. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr Clin North Am. 2017 Dec;40(4):739-749. doi: 10.1016/j.psc.2017.08.008. Epub 2017 Sep 18. PMID: 29080597; PMCID: PMC5679245.
Tan, Z.Y.A., Wong, S.H., Cheng, L.J. et al. Effectiveness of Mobile-Based Mindfulness Interventions in Improving Mindfulness Skills and Psychological Outcomes for Adults: a Systematic Review and Meta-regression. Mindfulness 13, 2379–2395 (2022). https://doi.org/10.1007/s12671-022-01962-z
Éva Gál, Simona Ștefan, Ioana A. Cristea, The efficacy of mindfulness meditation apps in enhancing users’ well-being and mental health related outcomes: a meta-analysis of randomized controlled trials, Journal of Affective Disorders, Volume 279, 2021, Pages 131-142, ISSN 0165-0327, https://doi.org/10.1016/j.jad.2020.09.134.
Goldberg, S. B., Lam, S. U., Britton, W. B., & Davidson, R. J. (2021). Prevalence of meditation-related adverse effects in a population-based sample in the United States. Psychotherapy Research, 32(3), 291–305. https://doi.org/10.1080/10503307.2021.1933646
Conrad A, Roth WT. Muscle relaxation therapy for anxiety disorders: it works but how? J Anxiety Disord. 2007;21(3):243-64. doi: 10.1016/j.janxdis.2006.08.001. Epub 2006 Sep 1. PMID: 16949248.
Jia Y, Wang X, Cheng Y. Relaxation Therapy for Depression: An Updated Meta-analysis. J Nerv Ment Dis. 2020 Apr;208(4):319-328. doi: 10.1097/NMD.0000000000001121. PMID: 32221187.
Köse Kabakcıoğlu N, Ayaz-Alkaya S. The effect of progressive muscle relaxation on stress, anxiety, and depression in adolescents: A quasi-experimental design. J Pediatr Nurs. 2024 Sep-Oct;78:89-96. doi: 10.1016/j.pedn.2024.06.014. Epub 2024 Jun 21. PMID: 38905787.